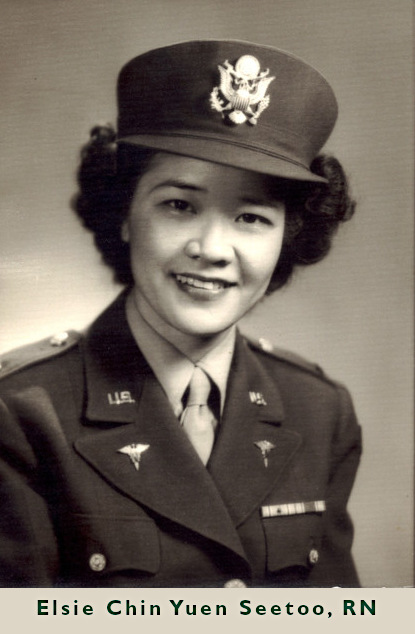
When Elsie Chin Yuen Seetoo was born on September 14, 1918, in Stockton, California, no one could imagine that by the time she was 30 she would work in a hospital under attack by the Japanese Army; escape occupied Hong Kong disguised as a Chinese servant; travel by boat, truck and foot across 700 miles of war-torn China; become the first Chinese-American nurse to join the US Army Nurse Corps; and then graduate from Women’s College in Greensboro, North Carolina, with a Bachelor of Science in Nursing degree. Her unique and harrowing tale begins decades before her birth.
Early Life
Seetoo’s father, along with thousands of other Chinese men, came to California seeking jobs and opportunities unavailable to them in their homeland. When he arrived, Mr. Chin first worked as a laborer and then as a cook for a private family. He saved enough money to open an import-export grocery store business in Stockton. He became a merchant because it provided the legal status he needed in order to bring his Chinese wife and son to the United States. After settling in Stockton as a family, the Chins had two daughters. Although she was the only Chinese student in her public-school classroom. she remembers her childhood fondly. The Chin children attended Chinese school from 5-9 pm, in Stockton’s small Chinatown, here they learned to read and write Chinese characters. In addition to her schooling, she was an active Camp Fire Girl (Lee, 2019)
In 1930 the United States was in the middle of the Great Depression. The family business was failing, so the Chins decided to return to China. Because Seetoo and her younger sister were born in California, they were United States citizens. After completing high school in China, she wanted to further her education. However, in the 1930s, Japan invaded China and controlled most of coastal and eastern China where the major cities and universities were located. Many Chinese universities closed during the Japanese invasion and occupation. In any event, the Chin family did not have enough money to help Seetoo with college expenses. So, in October 1938 she began her studies at the English language Queen Mary Hospital School of Nursing in the British Colony of Hong Kong (Moy, 2014).
Student Nurse Days
On December 7, 1941, the Japanese attacked Pearl Harbor, bringing the United States into World War II. That same day Japan also attacked the Philippines, Hong Kong, Burma and other Asian countries. Seetoo recalled:
“… it was the morning of December the eighth, when we were greeted by Japanese bombs and shelling. Of course, we were placed on a wartime footing right away … All patients that could go home were sent home, and then we were taking in battle casualties that very first morning … after two weeks Hong Kong surrendered … we knew after that the Japanese are going to want the hospitals … the British sisters [nursing faculty] had the foresight to know that they were going to be interned, so they gave us our temporary certificates, RN certificates. (Trojanowski, 2005).”
On December 10, 1941 during the Battle of Hong Kong, nursing school administrators issued each third-year student a Certificate of Training from the Medical Department of the Government of Hong Kong. These certificates were on par with diplomas and conferred the title Registered Nurse (Chung, Ching & Wong, 2011). Chinese, British, Indian and Canadian forces defended Hong Kong during two weeks of fierce fighting. Facing overwhelming Japanese forces, the allies surrendered on Christmas Day, 1941. By then, Queen Mary Hospital was full of casualties. Seetoo, alongside hospital staff and fellow student nurses, worked tirelessly caring for the wounded soldiers. On December 26, 1941, Japanese Army troops entered the hospital, interned the foreign patients and staff, and turned the hospital into a Japanese Military Hospital (Copp, 2001). Seetoo was 23 years old, a Registered Nurse and living under Japanese rule in occupied Hong Kong. In an oral history interview she remembered:
“A few days after the surrender we saw some Japanese officers come to inspect the hospital … as soon as we saw them, we were kind of on edge, because you’d hear all these stories about rape, and rape of Nanking, and the Japanese had been very bad about commandeering women to be part of their—they called it comfort women, which is actually making sex slaves of them. Anyway, we had heard stories of that, so naturally we were very, very concerned.” (Trojanowski, 2005).
Rita Wong, one of Seetoo’s classmates, remembered the early days after the Japanese invasion,
“All foreigners working at the hospital were sent to a concentration camp, and the Chinese were gathered at a hospital where they had nothing to do but wait for their meager food rations. The Japanese made it a rule that no doctors or nurses were to leave Hong Kong, and those who were caught doing so would be killed.” (Macfie, 2007, p.1)
Escaping Hong Kong
Despite this Japanese edict, Seetoo and several of her Chinese classmates, including Rita Wong, Rebecca Chan Chung, Daisy Pui-Ying Chan, Cynthia Chan and Irene Yu, were determined to help their country and its American and British allies. They knew they had to make their way to Free China, which was in southwestern China and unoccupied by the Japanese. Individually and in small groups, these nurses disguised themselves as peasants and slipped past Japanese guards as they escaped from Hong Kong, making the 700-mile journey inland towards Kunming, the capital of Free China (Chung, Chung & Wong, 2012).
Seetoo, her brother and three of her classmates began the journey together. They traveled to Macao by boat, then hitched a ride with a truck driver to the Chin family home in Xinhui. After a short visit, the group walked four hours to Shuiko where they boarded a ferry. On the ferry was a classmate of Seetoo’s brother, Mr. Liao. She recalled their encounter:
“[Mr. Liao said] I’m going to write a letter to the pastor of the Baptist Church at your next stop, Gaoyao, and ask him to let you folks sleep in the church sanctuary – and to provide whatever assistance you need. And when you leave for the next stop, ask him to write a letter to the Baptist preacher there in Wuzhou asking for the same favor … That was how we finally got to Guiyang – by stopping at various churches along the way.” (Trojanowski, 2005).
In April 1942 they reached Guiyang, headquarters of the Chinese Red Cross Medical Relief Corps (CRCMRC). There she met Dr. Robert Lim, the director of the organization, who offered her a position in the operating room of the Red Cross sponsored hospital in the city. Seetoo accepted the offer and went to work.
Crooks has published a paper, titled “The Impact of COVID-19 Among Black Girls: A Social-Ecological Perspective,” in the Journal of Pediatric Psychology, reporting on the findings of a qualitative study that featured interviews with 25 Black girls—ages 9 to 18—from December 2020 to April 2021. Most participants reported significant psychological and physical consequences, including depression and anxiety, disrupted eating, distorted body image, and changes in self-esteem.
“Black girls are a very vulnerable and unprotected population, especially within the context of COVID,” Crooks says. “I thought it was a really critical question to be asking youth: How has this impacted their perceptions of self?”
Black girls are particularly vulnerable because they enter puberty and develop secondary sex characteristics earlier than their non-Black peers, according to the paper, causing them to suffer from “adultification” and “sexualization by society.” This can lead to elevated sexual and mental health risks.
Crooks found that only two of the girls in the study received any formal sexual education during the pandemic, as schools opted to delay teaching sex education during online learning due to the sensitive nature of the topic.
“Missing such a critical component of education was alarming to me,” she says. “This is a critical period in their life. Just because the world stops, doesn’t mean their bodies stop growing and evolving.”
Social media also played an outsized role in the girls’ lives as they found themselves isolated from peers during quarantine. Some girls struggled with body image issues and eating disorders, Crooks says.
“They were sitting in their houses watching TV, or they were on social media sites like Instagram or Tik Tok, so they were constantly exposed to overly-sexualized, unrealistic expectations for what their bodies are supposed to look like,” Crooks says.
Conversely, a majority of the participants said the isolation and reduction in peer interactions allowed them to engage in emotional healing and self-discovery, independent from peer pressure.
The pandemic also intersected with the Black Lives Matters movement. As the participants increasingly turned to media in lieu of social interactions, they saw mistreatment of Black people by police, including the murders of Breonna Taylor and George Floyd, nationally broadcasted. These messages led to mixed feelings among the participants.
“A lot of what the girls talked about was feeling empowered to be Black and having a sense of pride within their identities,” Crooks says. “On the other hand, there was fear that came with color of their skin – fear of being harmed themselves, or their fathers, brothers or other family members being hurt. There was this constant fear and threat to Black families.”
Crooks says her research shows the need for more school-based programming to bridge the gap in sexual health education in schools, as well as the need for family interventions to instill protective strategies in Black girls to help them be prepared to handle threatening situations.
According to the National Institutes of Health’s National Institute of Drug Abuse, researchers have determined that drug abuse and overdoses have increased during the pandemic. For an addictions nurse, this isn’t surprising. It’s an incredibly stressful time. And more stress results in more cravings for those struggling with addiction.
Hughes took time to answer our questions about being an addictions nurse.
Stephanie Hughes, MSN, APRN
How did you get interested in being an Advanced Nurse in the addiction treatment field? What drew you to it? How long have you been doing it?
My nursing career started in 1998. My first job was in a Behavioral Medicine Unit at King’s Daughters Medical Center in Ashland, Kentucky, where I cared for patients with substance use disorders. I learned how the disease of addiction affects the entire family unit as well as loved ones, and how addiction is unbiased toward socioeconomic status, level of education, or age. This disease affects people of all walks of life.
In 2002, I became the nurse manager of this unit. My leadership role at this medical center extended to the Pre-operative Cardiac Catherization/Intervention Unit. It was approximately two years later when I realized my love for behavioral medicine and returned to it. In 2008, I completed my Master’s in Nursing with an emphasis on leadership and education. This led me to serve as an adjunct clinical instructor at Ashland Community and Technical College, where I worked with RN students in their Psych rotation. I now have been a nurse for 23 years and the disease of addiction along with dual diagnosis (depression, anxiety, PTSD/trauma) continues to be my passion and calling. I continue to learn every day from colleagues and mentors, and, most of all, my patients.
Explain to me briefly what you do as an Advanced Nurse in addiction treatment. Did you have to get additional training/education to do it?
In 2014, I graduated from Frontier Nursing University in Versailles, Kentucky, with a post Master’s degree as a board-certified family nurse practitioner. I also am a buprenorphine waivered practitioner, which means I can prescribe one of the three FDA-approved medications used to treat opioid use disorder. To become waivered, you have to be a qualified practitioner, such as a nurse practitioner or clinical nurse specialist, and apply through and be approved by the Substance Abuse and Mental Health Services Administration (SAMHSA). It also helps to have practice experience in the different levels of care for substance-use disorders, from detox, residential, and partial hospitalization to intensive outpatient and outpatient opioid treatment programs. Having worked in the full continuum allows me to truly meet patients where they’re at and willing to accept care.
What types of people/clients do you serve?
Together with a specialized medical and clinical team, I serve adult men and women who suffer from substance use disorders and their families. Patients who seek treatment for addiction to drugs or alcohol are looking for the same thing any other patient is looking for—they want to be seen by qualified professionals who are engaged with them and they want to be treated with dignity and respect. It’s no different than in a hospital or other care setting; our patients appreciate and remember a friendly smile, a warm blanket, a hot meal, and their hygiene needs being met. As a nurse, I think it’s very important to remember that basic needs are just as important as passing medications and medical treatments. Many of our patients come to us lost or forgotten. Some are homeless, jobless, or estranged from their families due to their addiction. But they still deserve our care, and we help them get their lives back. The treatment we provide not only heals their brains and bodies, but gives them life skills, coping skills, and relapse prevention strategies. And we connect them to other resources in the community as well as our own alumni recovery network for support.
What do you like most about working as an Addictions Nurse?
I get to be the friendly face that greets patients during their first days of treatment. Some days I work to physically stabilize patients and treat the symptoms of detox, and others I just offer a calm, compassionate atmosphere and listen to my patients. Seeing the freedom of recovery through my patients is absolutely amazing. These individuals are some of the strongest people I have ever had the pleasure of meeting. The work they put in to their recovery is unfathomable to many.
What are your biggest challenges in this position? What are your greatest rewards in it?
The biggest challenge for me is having an up-close and personal view of the effects of this terrible disease. One exacerbation/relapse could very well result in death. The loss of so many lives is absolutely devastating.
The greatest reward for me is seeing patients who are working hard and making progress in their recovery—like seeing a patient who now has a relationship with their children and family. They may have gained employment and are able to live independently. I get to help people who will continue to work on their recovery and do amazing things. Many will stay in this field and go on to help others. It’s an amazing dynamic.
What advice would you give to someone considering this type of nursing work?
Nurses who care for people suffering from substance use disorder must empathize with our patients and families. When nurses are able to practice empathy, they are able to treat their patients as people, not diseases, and focus on a person-centered care approach.
Treatment is personalized for each patient. This is not cookie cutter treatment. Being a team player and having good communication is critical. Personalized treatment is delivered through a multi-disciplinary treatment team approach with the patient being the focal point. Many patients enter treatment confused, disoriented, and emotionally defeated. We must be the voice of our patients during these times. We as nurses have to have a strong passion for patient advocacy. This ensures we are always fighting for the very best care for our patients.
The recent news of elite Olympic athletes prioritizing their mental health and their own physical wellness over their sport has focused a national spotlight on the complexities and the prevalence of mental health struggles. And while seeing people who are suffering from mental health issues is difficult, the athletes’ public struggles have opened a door that allows healthcare providers to raise the issue with patients and loved ones.
In some minority communities, mental health struggles remain taboo to discuss openly. People who are experiencing symptoms of illness such as depression, anxiety, or obsessive-compulsive disorder, or even life-threatening suicidal thoughts face a stigma that prevents them from even seeking care. When the issues are discussed, access to affordable and high-quality mental health providers can be a barrier to getting help, as can lack of insurance and any language barriers.
According to the OMH, mental health is a serious and common health issue with approximately 18 percent of the entire U.S. population having a diagnosable mental illness within any given year. Of that percentage, only 43 percent of people who need mental health care receive treatment or counseling. For minority mental health needs, the numbers are even more concerning. While 48 percent of whites receive care, only 31 percent of Blacks and Hispanics do. And statistics for Asians were even lower at just 22 percent receiving needed mental health services. Disparities in mental health care can lead to lack of treatment or ineffective treatment.
For most people, mental health treatment is effective and improves their quality of life. Whether people choose medication (psychiatric nurse practitioners are especially), talk therapy, or a combination of both, getting help can make symptoms abate significantly. In more transient cases of mental illness, for example depressive symptoms caused by a major life change, treatment can get someone back to feeling like their old selves and can improve their resiliency moving forward.
These care disparities have lasting impact. According to the American Psychiatric Association minority and white populations have similar rates of mental illness, with white populations being slightly higher in some instances. But when Black and Hispanic people have depression, for example, the effects are more persistent. And systemic racism plays a role in proper care. The report states that “Racial/ethnic minority youth with behavioral health issues are more readily referred to the juvenile justice system than to specialty primary care, compared with white youth.” If mental health needs aren’t addressed and youth don’t receive proper care, that can lead to a disciplinary cycle that impedes educational and employment opportunities.
As a healthcare provider, keeping conversations about minority mental health open and ongoing with patients and having easily accessible resources available can make all the difference to helping patients get the care they need. From understanding the different types of mental health professionals and what they do to addressing medications or alternative therapies in a comprehensive treatment approach can help patients understand the range of help available. And with a recent uptick in the availability and acceptance of virtual therapy appointments, accessing care is somewhat easier for people.
Raising awareness and broaching the topic about minority mental health is important to removing the stigma and helping people move toward care that works for them.
There’s no questioning the difficulty of a career as a nurse. You may have to work long hours, deal with a variety of patients each day, and spend most of the time on your feet. You also have to deal with the risk of things like patient violence or the general sadness that comes from losing a patient you’ve been working with. But, nursing can be an incredibly rewarding career when you’re in the right work environment. A toxic work environment, however, is a different story. It can make getting your job done feel nearly impossible. If you come home each day feeling absolutely drained, and perhaps even frustrated or helpless, you might be dealing with a harmful environment at work.
So, how can you know what a toxic work environment looks like? What are your rights, as a nurse, to a healthy environment, and what can you do to make sure those rights are upheld?
What Does a Toxic Work Environment Look Like?
As a nurse, you probably already understand the importance of being able to adapt to different work cultures. If you’re not sure how to learn more about a specific culture or atmosphere within a workplace, there are a few things you can do to get a feel for it quickly, including:
Watching and learning from others
Asking questions
Staying transparent
The more you observe and the more questions you ask, the easier it can become to see if you’re dealing with an unhealthy work environment. Bear in mind that if you don’t like your job or you’re not satisfied with your work, that doesn’t automatically mean you’re in a toxic environment. You may need to try a different career path. But, toxicity in the workplace is very different. You can recognize it through some of the following signs:
There is an overall lack of communication
There are cliques, exclusions, or groups
The workers aren’t motivated to do their jobs
Growth is discouraged
Everyone is burnt out
Finally, there’s nothing wrong with going with your gut. If you get a “bad” feeling about your workplace, even if you can’t quite put your finger on it, don’t ignore those feelings.
How Can It Affect You?
A toxic work environment is more than just an inconvenience. It’s more than just something to “trudge through”. In fact, an unhealthy work environment can contribute to a variety of physical and mental health issues. Some of the most common problems include:
Fatigue
Upset stomach
Heart issues
Muscle aches
High blood pressure
The toll on your mental health is nothing to take lightly, either. You might find yourself constantly feeling stressed and overwhelmed at work. It doesn’t take much for that to carry into your home life if you can’t let the feelings of the day go when you walk in the door. That constant feeling of stress can lead to mental health conditions like anxiety, or even depression. As that continues, you may end up needing to get extra help just to deal with those conditions.
Working every day in a toxic environment can wear you down. So much so, that it can even weaken your immune system, making it easier to get sick. As a nurse, you know the importance of taking care of your mind and body. If you don’t make self-care a priority, it could impact your personal life in a negative way. Your work environment shouldn’t be the thing that compromises your health.
How to Find a Healthier Environment in Your Field
If you find yourself in a toxic work environment, the best thing you can do is leave. An environment that large isn’t likely to change, even if you address the issues. You need to prioritize your needs when it comes to your career and your overall well-being. But, leaving a job isn’t always easy if you need the income.
Waiting to leave until you have another job lined up is always a safer option. Or, you might consider going a more nontraditional route with a remote job. Remote jobs allow you to work from home (or anywhere!), eliminating everything from toxic employees to negative patient interactions. Working remotely can help to reduce your stress levels and offer more flexibility.
Obviously, not all nursing jobs are able to be done remotely, but there are some that will allow you to work from home while still caring for others, including:
Clinical appeals nurse
Health informatics
Nursing instructor
Nurse auditor
Telephone triage nurse
Some larger hospitals and even national health care groups are always looking for nurses who can work remotely and fulfill these needs. These particular jobs might be different from what you’re used to, but that could be exactly what you need to break free from a toxic environment. In doing so, you can learn to enjoy your work again, and find fulfillment in helping patients while taking care of yourself, too.