Cultural Competence Is Essential in Diabetes Care
As rates of diabetes continue to rise, endocrine nursing is a specialty that will continue to have a pressing need.
Diabetes care is only one aspect of an endocrine nurse’s specialty—thyroid disorders and adrenal gland disorders also are endocrine system problems—but November’s designation as American Diabetes Month highlights this particular condition.
An endocrine nurse can choose to work with adult or pediatric patients, and they will see different presentations of the same disease across all populations. Because diabetes can present in varying ways for each individual and treatment plans can differ widely, an endocrine nurse must have a broad expertise in how diabetes impacts many body systems.
Cultural competence is especially important in this nursing specialty as traditions around food alone—eating, feasting, or fasting—will have an immediate and potentially dangerous impact on someone with diabetes.
Diabetes is so prevalent today that most people know of someone who has Type 1, Type 2, or gestational diabetes. The different types of diabetes stem from separate issues, but result in the same inability to use insulin.
According to BeyondType1.org, these are the more common forms of diabetes:
- Type 1 is a chronic autoimmune disorder that seems to have genetic and environmental causes and is something that cannot be prevented.
- Type 2 is when the body is unable to use insulin (also called insulin resistance). This type has several causal factors including lifestyle factors like obesity, inactivity, or smoking, but there’s some research that notes a genetic cause for some minority populations with Type 2.
- Gestational diabetes happens during pregnancy when hormones can interfere with the body’s normal use of insulin.
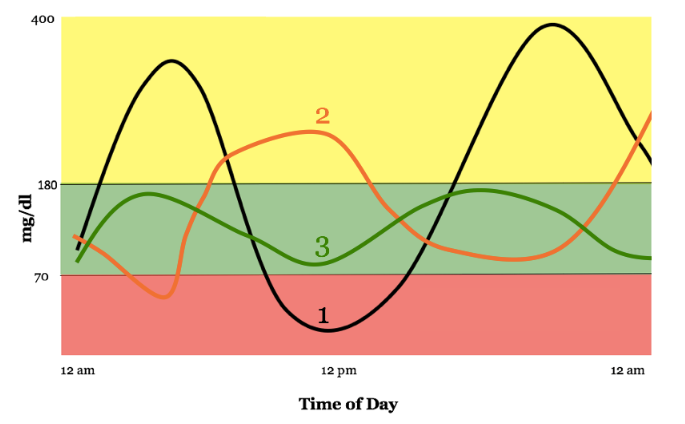
Like many chronic conditions, diabetes has a direct and significant impact on a person’s daily life and activities. Blood sugar rises and falls throughout a normal day, but other factors like an illness, stress, or travel can pose particular challenges for people with diabetes. They need to be vigilant and prepared for any red flags in their insulin numbers.
As an endocrine nurse, you’ll need to help your patient put the pieces of their personal diabetes puzzle together and then take it apart to examine all the factors that could change their typical treatment. Understanding your patient’s cultural norms will go a long way to developing a diabetes plan that will work and that the patient can and will follow.
Diabetes management will look different for each person, but it’s helpful to ask questions that might reveal religious or lifestyle preferences and choices that could play a part in how they can manage their condition. Children and teenagers can be particularly challenged by social pressures to keep on track. And many patients, young and old, go through a period of denial when they think they don’t need to worry too much about their disease. If you’re a nurse with diabetes, you know the challenges first-hand.
Educating patients about the severe complications that can arise from mismanaging this condition, no matter what type it is, is essential. But it’s also important to let people know how the diagnosis of a chronic condition like diabetes can cause changes in mental health and that help is available. You can share resources about the diabetes communities—both online and local—so that patients can learn from others and know they aren’t alone.
Endocrine nurses have the responsibility of helping patients follow their treatment plans and of having the compassion to understand why it is so hard to do. Nurses who understand their patient populations have an advantage, so learning as much as you can about the cultural norms will help.