Shifting demographics and other market conditions have created a greater need for minority nurses, particularly in certain roles. With a growing multicultural and aging population in the United States, the need for medical case managers to serve patients of various ethnic and minority groups has significantly increased. Regulatory reform—specifically, the enactment of the Patient Protection and Affordable Care Act, which ushered in new preventable readmission requirements for hospitals, along with new models of care (e.g., patient-centered medical homes and physician-hospital organizations) and more prevalent consumer-driven health care plans—has created new opportunities for minority nurses in case management. For minority nurses whose goals are to help serve these largely underserved patient populations and advance in their careers, it is important to understand the changing health care landscape.
Let’s look first at our nation’s changing demographics. The graying of America has resulted in more Americans living longer with more age-related, chronic medical conditions, ranging from arthritis, hypertension, and heart disease to hearing impairments and cataracts. According to the National Academy on an Aging Society (NAAS), almost 100 million Americans have chronic conditions, with millions more developing chronic conditions as they age. By 2040, the NAAS estimates that the number of people in the United States with chronic conditions will increase by 50%. The cost of medical care for Americans with chronic conditions could approach $864 billion in 2040—almost double what it was in 1995. While the most common chronic conditions are the same for blacks and whites, the conditions are generally more serious among minority populations, particularly individuals with lower incomes.
Another major factor in our changing health care landscape is the higher percentage of racially and ethnically diverse individuals. An AARP Bulletin article titled “Where We Stand: New Realities in Aging” reported that minorities are expected to comprise 42% of the American population by 2030. Currently, the United States has 150 different ethnic cultures represented within its population, with over 300 different languages spoken and a wide range of cultural nuances reflected. For health care providers, this broad spectrum of cultural diversity in its patients introduces higher incidences of certain conditions, while also posing challenges relating to care and communications.
Addressing Cultural Challenges
On the disease front, we know that certain ethnic groups are more prone to certain medical conditions. Many health care providers and insurers are responding with targeted initiatives, such as: the Chinese Community Health Plan’s Diabetes Self Management: A Cultural Approach initiative to enhance diabetes knowledge and management in the Chinese population; Excellus Health Plan’s Healthy Beginnings Prenatal Care program to decrease NICU admission rates for African American teens; and Med One Medical Group’s Adherence to Hypertension Treatment and Measurement project to educate English, Arabic, and Vietnamese-speaking hypertensive patients.
Beyond the obvious language and communication barriers that can prevent quality health care delivery and optimum patient outcomes, there are cultural issues that, if mismanaged, can also interfere with providing quality health care. For example, in Latin culture, religious healing, praying to certain saints, and relying on religious symbols to address health issues are not uncommon. Patients of African descent are inclined to believe in the healing power of nature and their religion. Within Asian groups, achieving balance between yin and yang, using certain herbs and foods, and relying on acupuncture to unblock the free flow of energy (chi) are common practices. Health behaviors also vary among ethnic groups. Armenians are tolerant of county health facilities, whereas the Vietnamese regard them and the related bureaucracy associated with government facilities as degrading. They, therefore, prefer receiving care in a physicians’ office, even if higher costs are incurred.
There also are differences relating to how certain minority and ethnic groups want to hear about their medical conditions. Did you know that the majority of African Americans and European Americans believe patients should be informed of terminal illnesses, while fewer Mexican Americans and Korean Americans agree? Family values relating to health care decisions also differ among minority and ethnic groups. Within the Mexican, Filipino, Chinese, and Iranian cultures, for example, there is the belief that a patient’s family should be first informed about a loved one’s poor prognosis so they can decide whether or not the patient should be informed. Obviously, these variables and many others are important for health care professionals to understand when caring for a patient. This is an area where minority nurses of different backgrounds and cultures can be a tremendous asset to their patients and to the overall health care system. Studies have demonstrated that case managers help strengthen primary care. This is particularly true when patients have complex or multiple medical conditions—as many elderly people do—or chronic conditions such as diabetes or chronic obstructive pulmonary disease.
Combating Disparities in Health Care
It is widely known that disparities exist in the care of minority patients. While this is more pronounced in rural primary care practices, it holds true across the board. An Institute of Medicine report found that “racial and ethnic minorities tend to receive a lower quality of health care than non-minorities, even when access-related factors, such as insurance status and income, are controlled.” Other studies also have explored these disparities, including Aetna’s “Breast Health Ethnic Disparity Initiative and Research Study” and Health Alliance Plan’s “Addressing Disparities in Breast Cancer Screening.” Collectively, they further make the case for minority nurse case managers to advocate for minority patients.
Related research supports the fact that, where minority case managers are in place, there is a significant improvement in patient outcomes. This was evident in a study of rural African American patients with diabetes mellitus where it was found that they were able to better control their blood sugar levels with a redesigned care management model, which incorporated nurse-led case management and structured education visits into rural primary care practices.
From Public Sector to Hospitals, Physicians’ Offices, and Entrepreneurial Settings
There is no question that, given today’s health care landscape, minority nurses have a great opportunity to help make a difference in the care of minority groups and enjoy heightened career fulfillment and potential advancement. Among the settings minority nurses can consider are:
• The public sector—serving within the Veterans Health Administration system for our veterans, many of whom are minorities, or the Indian Health System for our nation’s native American populations;
• Hospitals—helping hospitals achieve lower rates of preventable hospital readmissions, caring for minority and ethnic patients, and serving as a patient advocate and liaison with family members;
• Physicians’ offices—facilitating patient-physician communications, assuring appropriate records are communicated between treating physicians, monitoring patients’ adherence to treatment plans, and identifying any family and/or home issues that might affect a patient’s well-being;
• Financial advisors and estate planning attorneys—working with these professionals who are becoming increasingly more involved in the financial aspects of their clients’ health care and the costs associated with their care, as well as protecting their clients’ estates;
• Independent practice—working for a case management firm or establishing your own practice.
Independent practices present an opportunity for minority nurses to shape their own destiny and financial reward. Through one’s own practice, a minority nurse can focus more fully on his or her patients’ well-being without the over-emphasis on cost containment we see in many other practice settings, especially hospitals. These nurses can decide that they want to specifically dedicate their practice to a certain minority and/or ethnic group. They can establish a truly patient-centered care management business model, performing health risk assessments, providing health coaching, disease education and management, assisting with patient transitions of care, coordinating health care resources on behalf of their patients, reviewing hospital bills, helping patients assemble their health records, and providing end-of-life care coordination.
Based on a 2013 survey by the National Council of State Boards of Nursing and The Forum of State Nursing Workforce Centers, nurses from minority backgrounds represent 17% of the registered nurse (RN) workforce. Currently, the RN population consists of 83% white/Caucasian, 6% African American, 6% Asian, 3% Hispanic/Latino, 1% American Indian/Alaska Native, 1% Native Hawaiian/Pacific Islander, and 1% other. Given the increasing shortage of nurses, combined with the growing demand based on our shifting demographics, it appears that the time has never been better for minority nurses, while fewer in number, to take center stage in case management.
Catherine M. Mullahy, RN, BS, CRRN, CCM, is president of Mullahy & Associates www.mullahyassociates.com, and author of The Case Manager’s Handbook, Fifth Edition.
Where nurses work, as well as their education level and specialty, can all influence how much they earn in salary. But all in all, respondents to the third annual Minority Nurse salary survey report making more this year than they did last year.
With rising salaries, the outlook for nurses may be getting brighter, but there are still some differences in pay by ethnicity.
Last year, nurses reported earning a median $68,000, and this year they reported an increase that brought their median salary to $71,000—a $6,000 jump over what they’d said they earned five years ago.
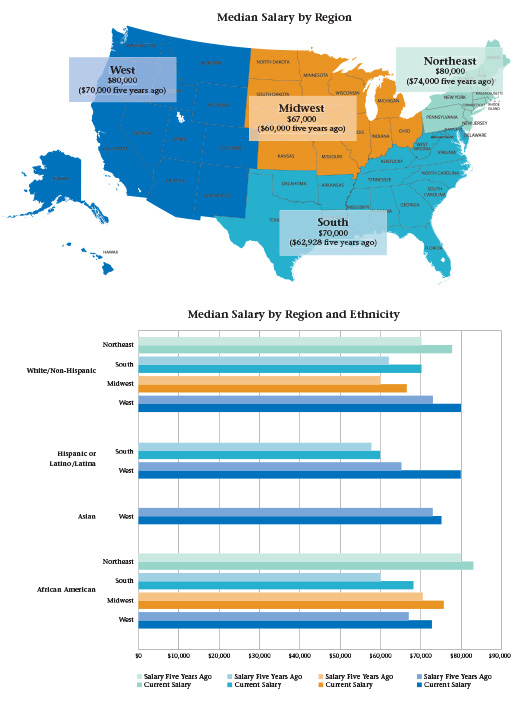
While African American nurses reported earning more this year than last, a median $60,200 in 2014 as compared to this year’s $70,000, they still took home slightly less than the overall median. Hispanic and Asian nurses said they earned slightly more than the overall median salary, and more than they reported earning last year, while white nurses reported a salary close to the overall median salary and similar to what they reported taking home last year.
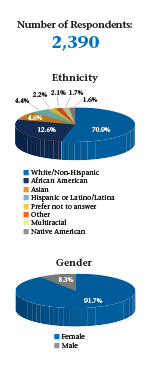
To collect this data, Minority Nurse and Springer Publishing e-mailed a link to an online survey that asked respondents about their jobs, educational background, ethnicity, and more.
Nearly 2,400 nurses from a variety of backgrounds and filling different job descriptions responded to the survey to provide a glimpse into their day-to-day roles, their plans for the future, and their current and past salaries.
The respondents work in various aspects of nursing from patient care to education and research, and have certifications in critical care, advanced practice nursing, and family health, among others. The nurses also work for a range of employers, from large organizations with more than 10,000 employees to ones with a hundred or fewer employees, and from public hospitals to colleges to home health care services.
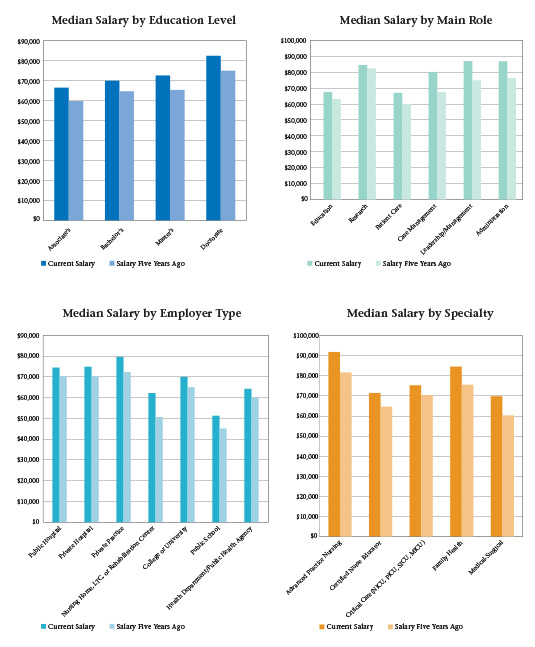
Drilling down deeper into the data, wider gaps in pay start to emerge. For instance, white nurses working at private hospitals earn a median $80,000, while African American nurses earn a median $62,000. Similarly, at public hospitals white nurses earn $79,500, and African American nurses $71,000. However, nurses employed by college or universities reported largely similar salaries falling between $70,000 and $80,000, with African American and Asian nurses reporting receiving the higher end of that range.
Salaries also vary by region in the United States. Nurses take home the most in the Northeast, followed by the West, though there also appear to be slight variations by ethnicity as white and Hispanic nurses living in the western US earn a median $80,000, while African American nurses earn a median $73,000.
Education also affects take-home pay, and nurses reported higher salaries with increased education. Nurses with associate’s-level degrees reported earning $67,000, while nurses with bachelor’s-level degrees said they earned $70,000. And that increased further with advanced degrees as those with master’s degrees reported taking home a median $72,000 and those with doctoral degrees said they made $82,000.
There, too, were slight differences by ethnicity. For instance, African American nurses with associate’s-level degrees reported taking home a median $65,119, less than the overall median, while white nurses took home a median $68,320, slightly more than the median. At the bachelor’s and doctoral levels, though, African American and white nurses reported earning approximately the same salary.
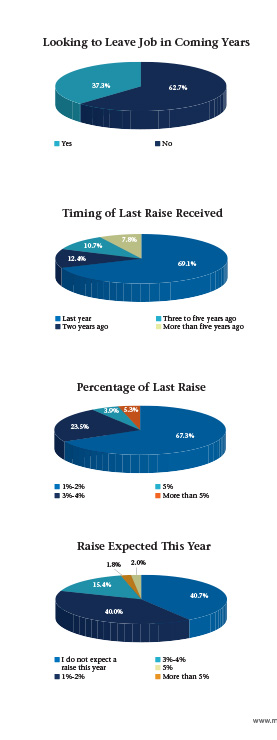
Despite rising salaries—and recent raises—more than a third of nurses still said they are contemplating leaving their current jobs in the next few years. When they left previous jobs, respondents said it was mostly to pursue better opportunities, and this year’s respondents reported that the best-paying places to work are in private practice or at private or public hospitals.
Inclusion tops the list of many workplace must-haves. But what exactly does inclusion mean?
According to G. Rumay Alexander, EdD, RN, FAAN, clinical professor and director of the Office of Multicultural Affairs at the University of North Carolina at Chapel Hill, when people talk about inclusion they can’t ignore one very important fact – inclusion means something different for each person.
“You have to define terms and explore it and explain it a little more carefully,” says Alexander, who recently moderated the American Nurses Association webinar Diversity Matters: Create an Inclusive Nursing Culture that Leads to Better Outcomes. “A prime example is that people talk about respect. The fact of the matter is that ten different people have ten different definitions of respect.”
How can you begin talking about inclusion?
1. Define It
Nurses excel at critical thinking skills, says Alexander, so sitting down to talk about what inclusion means in your workplace should be the first step.
2. Think About What Inclusion Means to You
“Self-awareness is so key to the work of an inclusive space,” says Alexander. “Understanding and knowing yourself is important. Know what pushes and doesn’t push your buttons.” Use honest self examination of your biases and prejudices so you become aware of them and realize how they could impact your work. Everyone has had different experiences, says Alexander, and each of those can change your outlook. The important work is understanding how that happens and making sure it doesn’t invade your work.
3. Be Willing to Change
When you do some honest reflection, you might realize where you need to make changes. That’s not a bad thing. Almost everyone needs to do something better, so having an open mind and understanding that you are part of a team trying to change takes the personal sting out. Be willing to learn. “Understand that your private decisions have public ramifications,” says Alexander. “You can’t talk your way out of what you behaved your way into.”
4. Change Your Culture
“Culture will trump strategy every time,” says Alexander. If everyone isn’t on board, any changes and any strategies put in place won’t hold. Understanding workplace culture means understanding who shapes the culture and how they interact. “You have to understand culture,” says Alexander. “Culture is the way you approach your work.”
5. Be Patient
“You have to understand when you are changing culture you are dealing with a process and that takes time,” says Alexander. A new environment won’t happen overnight, but it will happen with self reflection, new approaches, and honest and open communication.
When sick and injured patients arrive at hospitals for treatment, they also bring with them their unhealthy prejudices and biases. On the frontline of health care and healing, nurses may find themselves dealing with patients who prefer a caregiver who is of the same race. Patients—or their loved ones—may express their racial preference with negative comments and intolerant behavior, or directly voice their desire for another nurse. In a perfect world, hospital management would not cater to racially biased requests or demands. But real life is imperfect.
One blatantly racist incident involving an African American nurse made national headlines in 2012 when a white, swastika-tattooed father demanded that no black nurse care for his sick baby at a Michigan hospital. That case served as a springboard for several lawsuits and as a template for health care providers of exactly what not to do. Tonya Battle, a 25-year nurse at Flint’s Hurley Medical Center, worked in the neonatal intensive care unit when she met the white parent. After introducing herself, she was told by him to get her supervisor. The father relayed his racial preference to the supervisor, who reassigned Battle.
According to the Lansing State Journal, Battle said that a note was posted on the assignment clipboard reading: “No African American nurse to take care of baby.” Hospital officials removed the sign from the assignment chart after a short time. Still, black nurses were not assigned to care for the infant for about a month “because of their race,” according to the lawsuit. Battle’s case has since been settled.
While such overt incidents are isolated, no one should be shocked by racist patients, says Roberta Waite, EdD, APRN, CNS-BC, FAAN, associate professor of nursing and assistant dean of academic integration and evaluation of community programs at Drexel University’s College of Nursing and Health Professions.
“Racism is prevalent within our society. At times it’s been more covert and other times it has been more overt. It’s much more covert now,” says Waite, although it depends on geographical areas. “The more shocking component is: what do we do about it? How do we talk about it? How do we work with our students if we work with them at all? And how do we have these discussions amongst our colleagues?”
Whatever the solutions may be for patients who discriminate against nurses based on race, physicians need them, too. A 2010 survey of emergency room doctors found that patients often reject the physician assigned to them and request a doctor of the same race, gender, or religion. Their requests are routinely accommodated. If the patient request came from someone who was female, non-white, or Muslim, it was more likely to be granted.
“It’s medicine’s open secret,” Kimani Paul-Emile, an associate professor of law at Fordham University, told The New York Times. Paul-Emile did not respond to Minority Nurse’s requests for an interview but has written extensively on the topic. “The medical profession knows this happens but doesn’t want to talk about it,” she wrote in an article in the UCLA Law Review titled “Patients’ Racial Preferences and the Medical Culture of Accommodation.”
So, how do nurses of color handle patient encounters they believe stem from bigotry?
For Stephanie Stith, RN, a travel nurse for the past 10 years of her 15-year career, staying calm is a coping strategy. “I just mainly look [at them]. I give myself some time, because it’s not worth losing a job for.” She recalled one experience involving a patient who told her he was a member of the white supremacist Aryan Nation. “He looked at me and said, ‘I hate niggers.’ I said, ‘Good, so do I.’”
No other nurse was available to treat him, so she assumed her medical duties. As she worked, he continued his racist rant until she reminded him it was not smart to deride the person helping him stay alive. “I wanted him to know that I have the power over your life, and you are calling me names? Not that I was going to do anything; I just wanted him to think,” explains Stith, who says she deals more with slights than outright racism. For example, patients sometimes assume she is a medical tech instead of a registered nurse because she is black.
Stith also refrains from becoming emotional when responding to racist patients. “I need a paycheck. It doesn’t benefit me to get indignant. You can call me ‘nigger’ and say whatever you want, but at the end of the week I cash my paycheck. I am contracted to perform a service. I can’t change anybody’s mind or attitude. All I can do is be the best I can.”
Retired nurse Dinah Penaflorida, RN, MPH, MSN, agrees. Her advice for new nurses dealing with such requests is to remember that “the patient’s comfort and trust comes first. It is more important to be patient-centered in the care than to take the patient’s request personally. When the patient is in pain and suffering, it is not the time to talk about race and discrimination.”
Penaflorida was born and raised in the Philippines. At 16, she received an American Field Service Scholarship to spend a year in Hutchinson, Kansas. As a staff nurse at Kansas University Medical Center in the 1980s, she encountered a few patients who requested a Caucasian nurse instead of her. When it occurred, she went to the charge nurse to comply with the request to “create a more comfortable environment for the patient to heal.” She left those experiences behind her when she moved to the West Coast. “Working in California was different. I did not experience that,” says Penaflorida.
Focusing on caregiving instead of the patient’s name-calling or other forms of intolerance is the best strategy, nurses say. “l always keep in the back of my mind that I had the best training going because I am a nurse of color,” says Deborah Bowser, RN, who has a master’s degree in health services administration and is a practice administrator in Richmond. “Most of my instructors were nurses of color and they dealt with worse situations than I have. They always instilled in us that ‘you will be judged by the color of your skin and it will be assumed you are not a RN, and you do not have the experience.’ They took no slack from us. We were the best of the best.”
Bowser recalled being rebuffed by two white patients during her 43-year career. Both incidents happened in New York during her night shift. Each time, her supervisor told the patient she was one of the best nurses. “One patient decided they did not want to be treated by me because I was black, so I informed my supervisor. The patient was extremely ill, so I said, ‘You have a choice; let your prejudices go by the side and let me take care of you. I know what I am doing.’ In one incident the patient said ‘yes,’ and in another the patient said ‘no’ and did not get care for a very long time because there was no other nurse who was Caucasian who could care for that patient.”
Bowser says she would like to think in this day and age that race-based requests would be nonexistent, “but you are going to have people who do not want people of color touching them” regardless of their expertise. For any young nurse of color who encounters such patients, “carry yourself with pride and get a mentor to help you,” she advises.
Racist patients can overwhelm young nurses, says LaDonna Northington, DNS, RN, BC, professor of nursing and director of traditional undergraduate studies at the University of Mississippi Medical Center (UMMC) School of Nursing. “A young nurse would probably be intimidated and wouldn’t know what to do but leave out of the room, so they have to find a mentor to help them… problem solve through a situation like that. A seasoned nurse is able to take a high road. If you try to take care of the patient, they can call it assault,” so a nurse must learn how to accommodate a patient from a legal standpoint, she explains.
“For a young nurse, they should get their charge nurse or head nurse to intervene. It’s a tough call,” says Northington, who has not dealt with a racist patient during her 35-year career.
“I can’t recall an incident when I was on the floor taking care of patients where I felt like a patient did not want me to take care of them because I was black…and you would think if it was anywhere blatant, it would be in the South where we are. I haven’t heard the students talk about it. It could be in pockets [of communities] or people deal with it in a different way.” The UMMC School of Nursing addresses sensitivity and cultural awareness and understanding, she says, adding it’s possible that black patients may reject white nurses. “An elderly black person who has never trusted white people because of Tuskegee and those kinds of things and Mississippi history” may request a black nurse.
Discussing race makes many people uncomfortable, but nurses say it’s part of the solution. “When you are talking about the elephants in the room, we talk more openly about religious differences… and gender or sexual orientation, but when you get to race, there is so much more hostility and changing the subject,” says Waite. “It’s not talked about openly… oftentimes not at all. I’m not shocked that those incidents occur; I am actually surprised it doesn’t occur more often.”
Waite uses a social justice framework to talk about such topics as power, privilege, oppression, “and every ism” in a leadership course she teaches all undergraduate health profession students, including nurses. “I explicitly talk about it. However, most often within nursing clinical courses the topic is called ‘cultural competence.’ That’s the catch-all phrase that overlays issues of culture and diversity. That phrase is probably in everybody’s syllabus; however, how each person operationalizes what they do in teaching their students will vary,” she says. It will come down to how comfortable that faculty member is in guiding or leading or discussing issues regarding race, she adds.
At the University of Texas-Pan American nursing department, the curriculum emphasizes culture and cultural differences among people, says Carolina G. Huerta, EdD, RN, FAAN, nursing department professor and chair. In one required course, undergraduate students spend at least two weeks listening to lectures and discussing the impact of culture on nursing care, with particular attention paid to debunking stereotypes and focusing primarily on each person’s uniqueness. The course aims to sensitize students to issues related to racism and stereotyping.
“Once admitted to our program, every student must address cultural implications of their nursing care following each of their clinicals,” explains Huerta. “There is a section on their assigned clinical paperwork that must be turned in that deals strictly with cultural implications of care. The students are asked to reflect on the patient that they cared for and address any cultural implications, whether these deal with the foods the patient ate, religious affiliations, overt or covert racism, family issues, et cetera.”
While some patients will always express a racial preference for nurses, what matters most is how the institution and administration respond to such requests. “If you cater and say ‘no black people will work with you,’ that’s the problem,” Waite argues. “A patient has the right to decide who will care for them, but they can’t do it in a discriminatory manner. Instead, the response could be ‘Everyone here is competent to take care of you. If you choose to [reject care from a specific nurse] that is fine, you can go to another hospital.’”
Most of the hospitals that have been in the news “gave in” to racial preferences, Waite notes. Hopefully, most hospitals have a statement within their policy on how to engage and work with clients if anything like this surfaces. Talking about these issues is key, she adds.
“I think oftentimes today, people think either you are racist or not. It’s not that you are racist or not; racism is a spectrum,” says Waite. “All of us continuously struggle to deal with prejudice and bias because no one is perfect. When trying to understand where these thoughts come from and not feed into it, we move society forward. And it’s going to move forward as we are able to have these open and authentic conversations with one another.”
Robin Farmer covers health, business, and education as a freelance journalist. Based in Virginia, she contributes frequently to Minority Nurse magazine and website. Visit her at www.RobinFarmerWrites.com.
Affirmative action has been a hot topic for decades. Since its tumultuous inception almost 50 years ago, affirmative action has been applauded, argued, and scoffed at as an answer to racial inequality.
In 1961, President John F. Kennedy was among the first to use the term “affirmative action” as a method to prevent further racial discrimination despite civil rights laws and, essentially, to temporarily level the playing field. Executive Order 10925 required that government contractors “take affirmative action to ensure that applicants are employed, and that employees are treated during employment, without regard to their race, creed, color, or national origin.”
But it was President Lyndon B. Johnson who developed and enforced it for the first time in 1965 with the passage of Executive Order 11246.
“This is the next and more profound stage of the battle for civil rights,” Johnson said to a Howard University graduating class in 1965. “We seek…not just equality as a right and a theory, but equality as a fact and as a result.”
Since then, the debate over affirmative action has grown more and more contentious and problematic as the public—with divided opinions—have weighed in on a complex issue.
Robert A. Schaeffer, the public education director of
FairTest, the National Center for
Fair & Open Testing, believes that many issues relating to race are highly controversial because critics have been able to define policies as “preferences” rather than “balancing” the playing field.
“Many Americans are convinced that affirmative action creates biases in favor of certain groups,” says Schaeffer. “Particularly in economic tough times, it is not difficult to fan resentment against any plan that seems to advantage [some] while disadvantaging others.”
Schuette v. Coalition to Defend Affirmative Action
In recent months, the battle over affirmative action once again gained momentum in light of the latest Supreme Court rulings. In April, the Supreme Court upheld a constitutional amendment Michigan voters approved in 2006, banning preferential treatment based on race, gender, ethnicity, or national origin in admissions to the state’s public universities.
By a vote of 6 to 2, the court concluded that it was not up to the judges to overturn the 2006 decision by Michigan voters to bar consideration of race when deciding who gets into the state’s universities and made it clear that states are free to prohibit the use of racial considerations in university admissions.
“This case is not about how the debate about racial preferences should be resolved. It is about who may resolve it,” Justice Anthony Kennedy wrote in an opinion joined by Chief Justice John Roberts and Justice Samuel Alito. “There is no authority in the Constitution of the United States or in this court’s precedents for the judiciary to set aside Michigan laws that commit this policy determination to the voters.”
Justice Sonia Sotomayor, on the other hand, blasted the majority, who she said attempts to “sit back and wish away” evidence that racial inequality exists.
“The stark reality is that race still matters,” Sotomayor wrote in her 58-page dissenting opinion joined only by Justice Ruth Bader Ginsburg. “The way to stop discrimination on the basis of race is to speak openly and candidly on the subject of race, and to apply the Constitution with eyes open to the unfortunate effects of centuries of racial discrimination.”
Moving Forward
It is unclear how the decision might move other states. Eight states, including Nebraska, Arizona, and Washington, now have bans on affirmative action. The ruling could encourage other states to join the handful that already have such prohibitions, such as California and Florida.
But what’s worrisome to proponents of affirmative action is the precedent that may have been set with the court’s ruling, potentially, further energizing opponents of racial preferences, who have already outlined plans to put Michigan-style constitutional amendments on the ballot in Utah, Ohio, and Missouri.
A survey conducted by ABC News and The Washington Post last year found that 79% of whites and 71% of non-whites oppose the consideration of race and ethnic preferences in college admissions, suggesting that any affirmative action ballot measures are likely to be voted down.
Moving forward, Roger Clegg, president and general counsel of the Center for Equal Opportunity believes that the court’s decision means that colleges in states that have banned racial preferences must follow those laws and other states without bans should reexamine with current plans.
“It also means that colleges in other states must take into account the fact that their continued use of racial preferences, which is unpopular, should consider getting rid of that policy since it may be banned in their states, too,” Clegg adds.
Quite the contrary, says Michael Olivas, director of the Institute for Higher Education Law and Governance at the University of Houston Law Center. “It hurt the choices that Michigan colleges wanted to make, and this violated their academic freedom.”
But it need not be a regressive process, Olivas continues. In Maryland, voters approved resident tuition for the undocumented in a ballot measure, and Colorado voters turned down a Michigan-type measure.
“They are neither good nor bad in and of themselves, except we should not make such important decisions for colleges by this means,” Olivas adds.
The groups that challenged the Michigan affirmative action ban pointed out the basic unfairness of giving preferences in admission to some groups while banning similar treatment of African Americans, Latinos, Native Americans, and women.
“Michigan higher education leaders and most major civil rights groups reinforced our arguments,” says Schaeffer, who provided expert assistance to the groups challenging Michigan’s ban. “However, the judicial system held that voters could impose whatever distinctions they determined to be reasonable.”
Impact on Minority Enrollment
What is not clear is the ruling’s impact on minority enrollment. While the US Supreme Court affirmed Michigan’s constitutional amendment banning race-conscious admissions, states that forbid affirmative action in higher education, like Florida and California, as well as Michigan, have seen a significant drop in the enrollment of black and Hispanic students.
In April 2014, The New York Times published an article examining how minorities have fared in states with affirmative action bans, including California, Florida, and Michigan. At UC Berkeley and UCLA in California, for example, the graphs showed that 49% of the state’s college-aged residents are Hispanic, though only 11% and 17% of freshmen are Hispanic at those two schools, respectively.
In Florida, 27% of the state’s college-aged residents are Hispanic at Florida State and the University of Florida, yet both universities showed that only 18% of their freshmen was Hispanic.
While the decision didn’t address the constitutionality of race-conscious admission policies, Justice Sotomayor cited student-demographic data as proof that the ban, which went into effect in December 2006, has adversely affected minority enrollment and diversity at the University of Michigan (UM) in Ann Arbor.
“A white graduate of a public Michigan university who wishes to pass his historical privilege on to his children may freely lobby the board of that university in favor of an expanded legacy admissions policy,” she wrote. “Whereas a black Michigander who was denied the opportunity to attend that very university cannot lobby the board in favor of a policy that might give his children a chance that he never had and that they might never have absent that policy.”
According to the policy brief, “Restructuring Higher Education Opportunity?: African American Degree Attainment after Michigan’s Ban on Affirmative Action,” which Justice Sotomayor cited in her dissenting opinion, the proportion of African Americans who obtained a bachelor’s degree at UM dropped by about one-third after the ban on race-conscious admissions went into effect.
Additionally, The New York Times article revealed that the enrollment of black freshmen at UM between 2006 and 2011 dropped from 7% to 5%, despite the number of black college-aged persons in Michigan increasing from 16% to 19%.
While Justice Sotomayor argued that the ban on race-conscious admissions might have had a negative effect on the number of minority students who enrolled, it has not necessarily stopped colleges from looking at alternative procedures to maintain and promote diversity.
A 2012 study by The Century Foundation, a nonpartisan group, found that at seven of 10 major schools where racial preferences could not be used, race-neutral alternatives helped maintain or even raise minority representation.
For example, Texas’s Top Ten Percent Rule—which guarantees admission to the University of Texas (or any state-funded university) to any high school senior graduating in the top 10% of his or her class—helps ensure diverse college student bodies. A combination of measures, including affirmative action based on class, increasing financial grants, and de-emphasizing standardized tests are just a few promising race-neutral options that have allowed minority enrollment to return to pre-ban levels.
“From FairTest’s perspectives, all these initiatives are worthy of consideration,” says Schaeffer. “But none fully replace affirmative action as a tool for addressing past and present discrimination.”
Fisher vs. University of Texas at Austin
Last June, the justices had a chance to make another big statement on affirmative action with its decision in Fisher vs. University of Texas at Austin (UT Austin). The case was filed by Abigail Fisher, a young woman from Texas who applied to the university but was rejected. Fisher, who is white, then filed a lawsuit, arguing that she had been a victim of racial discrimination because minority students with less impressive credentials than hers had been admitted.
The Supreme Court did not immediately decide the fate of Fisher. Instead, the justices voted 7-1 to return the case to the lower courts to determine whether the use of race is “necessary” and have “the ultimate burden of demonstrating, before turning to racial classifications, that available, workable race-neutral alternatives do not suffice.”
“Strict scrutiny must not be strict in theory but feeble in fact,” Justice Kennedy wrote. “The reviewing court must ultimately be satisfied that no workable race-neutral alternatives would produce the educational benefits of diversity.”
Only Justice Ginsburg dissented in the decision to send the case back.
“I would not return this case for a second look,” Ginsburg wrote in her dissent. “The University reached the reasonable, good-faith judgment that supposedly race-neutral initiatives were insufficient to achieve, in appropriate measure, the educational benefits of student-body diversity.”
The ruling upheld Gratz v. Bollinger and Grutter v. Bollinger, two cases fundamental in defining universities’ rights to consider race as an admissions factor. Though many argue that the court’s decision preserves the principle that affirmative action is permissible in some circumstances. That, according to Olivas, depends upon the narrow tailoring that the remand requires.
“UT Austin is allowed to use race (by Grutter), and the top ten percent plan—which I helped write—is race-neutral, so Fisher was not harmed. She was simply not admissible,” Olivas argues. “The plan allows in over 50% whites, in a state where whites are only 30% of the [high school] population. It does not harm them, nor does the modest affirmative action policy.”
It can be said both decisions illustrate the court’s skepticism about race-conscious government programs. The Schuette v. Coalition to Defend Affirmative Action ruling alone took five separate opinions totaling 102 pages written over six months—a sign of how divided the court remains on the issue and the role the judiciary should play in protecting racial and ethnic minorities.
To most, the recent Supreme Court’s decision upholding Michigan’s affirmative action ban was far from a shock, but many believe the ruling could symbolize a steady march to the end of the use of race in higher education.
But, for now, the most recent Supreme Court decision only impacts public colleges and universities in the state of Michigan. The voter-approved Constitutional amendment clearly bars them from considering race, gender, ethnicity, or national origin in admissions and related decisions.
“For higher education institutions in other jurisdictions that are not operating under similar bans [some states, such as California, have their own prohibitions], affirmative action policies that comply with the court’s Hopwood [v. Texas] and Grutter decisions remain legally permissible,” says Schaeffer. “However, many who closely observe the Court believe that further restrictions on affirmative action are likely as the result of Fisher and other cases, currently moving through the judicial system.”
Terah Shelton Harris is a freelance writer based in Alabama.
Racially and ethnically diverse populations have grown in the US. The US Census Bureau finds that approximately 37% of the population is made up of minority groups. Nurses currently make up the largest group of health care professionals in the US, and the need for culturally diverse nurses in the workplace has been identified by many nursing leaders. The demand for culturally competent care has brought attention to the need for culturally diverse nurses. Several studies have identified that failure to provide culturally competent care can influence health outcomes. A 2009 study published in Health Affairs found that increasing minority representation in the health care workforce could have a positive effect on curbing the health care disparities found in minority populations.
The need for culturally competent health care highlights the need for a diverse nursing workforce, particularly since patients tend to migrate towards providers that share their ethnic background. Minority nurses and possibly advanced practice nurses are in a position to help these often underserved minority communities receive care that will increase their likelihood of compliance with medical treatment and increased health literacy.
Additionally, implementation of the Affordable Care Act will allow for the expansion of health insurance to historically underserved populations. This expansion will require an increase in the number of health care professionals available to care for these populations.
Of the almost 3 million registered nurses in the US, approximately 133,000 are black and 55,000 are Hispanic. A 2013 study published in Journal of Transcultural Nursing reveals that minority students account for about 27% of the students in undergraduate schools of nursing. The low number of minority students represented in the undergraduate nursing school enrollment numbers highlights the difficulty noted by graduate schools when it comes to attracting and enrolling minority registered nurses.
Federal initiatives like the Promoting Postbaccalaureate Opportunities for Hispanic Americans program authorized under Title V of the Higher Education Act of 1965 are designed to expand postbaccalaureate opportunities and academic offerings for universities that are educating the majority of postsecondary Hispanic students. According to a 2010 brief published by Excelencia in Education, there were 176 emerging Hispanic-Serving Institutions (HSIs) in 2007. Federal law requires that in order to receive a designation as a HSI, an institution must have at least 25% Hispanic undergraduate enrollment. Emerging HSIs are those with Hispanic enrollment within the range of 12% to 24% and have the potential to become HSIs over the next few years. The HSI designation allows an institution to qualify for grants and other modes of funding. A 2010 study published in Journal of Latinos and Education found that, behind funding, the most important issue facing the presidents of HSIs was the lack of academic preparedness of the students.
Challenges are faced by Hispanic nurses desiring to pursue advanced nursing degrees. Like undergraduate enrollment, the number of registered nurses with baccalaureate degrees applying for advanced practice nursing tracts is low. There are four HSI institutions that offer nurse anesthesia in these fine programs: University of Miami, Kaiser Permanente / California State University, Inter-American University of Puerto Rico, and the University of Puerto Rico. A relatively large Hispanic applicant cohort of prospective students submit to these diverse nurse anesthesia programs along with other urban located institutions within the US. A barrier that some underrepresented students encounter is the lack of academic preparedness and/or lackluster graduate exam scores. This lack of academic preparedness equals fewer applicants who are adequately prepared for undergraduate and graduate education. In the event that a student is successful in an undergraduate program, lack of preparedness could lead to the preparation of a graduate application packet that is not representative of the candidate’s true potential.
Optimization of the nurse anesthesia program application packet can mean the difference between acceptance and rejection. The graduate application for nurse anesthesia school normally contains many components. The application is the first glimpse of the candidate presented to the admission committee. One crucial component of the process is the essay. The essay should contain information that the candidate wants to express describing his or her participation in leadership and extracurricular activities. Admission committee members take note of well-rounded candidates. Candidates should include evidence of involvement in professional nursing organizations and hospital committees. These types of activities highlight the candidate’s desire for professional development. The essay should be edited for grammar, spelling, and content before the packet is submitted to ensure that the candidate appreciates attention to detail.
The construction of a comprehensive application will most likely yield an interview, but the interview process can be intimidating. Most admission committees attempt to evaluate the student’s preparedness for the rigors of the program. The types of questions revolve around principles of physiology, pathophysiology, and pharmacology. Candidates who recognize their deficiency in interviewing should seek out opportunities to practice these techniques. Career centers may offer opportunities to hone interviewing skills.
Prospective students tend to focus on securing a seat in a nurse anesthesia program, but it is unclear how many actually consider the rigorous nature of the program. The amount of preparation that goes into the admission to a nurse anesthesia program is only minimized by the challenges of the didactic and clinical experiences for a new student. These challenges should be considered in conjunction with other stressors that can include financial obligations, reduction of income, and family responsibilities.
How to Strengthen your Application and Secure an Interview
According to the American Association of Nurse Anesthetists (AANA)’s 2012 demographics of nurse anesthetists in the United States and Puerto Rico, as an aggregate number, there is less than 10% of underrepresented minority nurse anesthetists from the 44,000 advanced practice nurses practicing in hospitals, surgery and endoscopy centers, and dental and pain management offices. Less than 3%, 3.2%, and 0.5% are from Hispanic, African American, and American Indian groups, respectively. To learn more about becoming a certified registered nurse anesthetist (CRNA), visit www.aana.com/ceandeducation/becomeacrna. Here, students will find information about the requirements of becoming a CRNA as well as a list of accredited nurse anesthesia programs, frequently asked questions, and a list of related published articles. It is imperative that prospective applicants into a nurse anesthesia program peruse not only the nurse anesthesia program of interest website, but also our national nurse anesthesia association website.
It is vitally important that underrepresented minority nurses learn more about the history of nurse anesthesia and national implications of advocacy. The book Watchful Care by Marianne Bankert is a great resource. It will expand your knowledge about nurse anesthetists and prepare you adequately for the interview, if the admission committee members ask any questions about this well-read topic. The top candidates definitely shine during the interview if they have read this material.
Another way to strengthen your application is to include your shadowing experience with a CRNA in the operating room. You should contact the CRNA and ask to meet him or her in the operating room on an agreed time. Be prepared to witness the CRNA prepare the room by checking the anesthesia machine and related equipment as well as prepare medications for the planned anesthetic prior to a patient’s arrival in the operating room. In addition, you will witness the CRNA interview the patient extensively about his or her medical and surgical history, review and secure the anesthesia consent, and perform an oral exam to assess a Mallampati score (I – IV) to anticipate an easy or difficult intubation prior to entering the operating room. During the shadowing experience, ask plenty of questions about what type of anesthetic is being administered (such as general, regional, or sedation), fluid management, positioning considerations, and more.
Along with learning the history of nurse anesthesia, as a critical care nurse with a baccalaureate degree, you should study and schedule the critical care registered nurse (CCRN) exam offered by the American Academy of Critical Care Nurses (AACN). Information regarding this exam can be found on the AACN website (www.aacn.org). This test demonstrates aptitude in critical care nursing and professional commitment towards excellence. A significant number of nurse anesthesia programs require applicants to earn critical care experience and sit for and pass the CCRN exam prior to actual submission of the essay for a nurse anesthesia program.
Another viable option for underrepresented minority nurses to improve the application process, handle the stressful interview, comply with the rigor of a nurse anesthesia program, excel for clinical preparedness, and learn about doctoral programs in nurse anesthesia programs is to register and attend Diversity CRNA Information Sessions & Airway Simulation Labs scheduled in 2014. This event, sponsored by the Diversity in Nurse Anesthesia Program (www.diversitycrna.org), offers an opportunity to those interested in nurse anesthesia education to fully engage oneself and learn comprehensive information about the process, network, and participate in a hands-on simulation experience in the lab. You will also have the opportunity and access to meet four nurse anesthesia program directors, AANA senior leadership, minority CRNAs, and nurse anesthesia students from across the country. As a result, you will have the ability to include details about your experience in your eventual essay and articulate it during your interview.
An additional application requirement of some anesthesia programs is the Graduate Record Examination (GRE). It is incumbent of any prospective applicant to visit the GRE website (http://www.ets.org/gre) to learn about the comprehensive information about the scores and the actual make-up of the exam (verbal reasoning, quantitative reasoning, and analytical writing).
So, now it is up to you. Will you peruse through the suggested websites to broaden your knowledge base about proper preparation for entry into nurse anesthesia? Do you want to be a competitive applicant for a nurse anesthesia program? Do you want to be academically and clinically prepared for such a program? If you answered yes to these questions, be proactive in your educational goals to advance your professional development in a nurse anesthesia program. You can do it!
Wallena Gould, CRNA, EdD, is the founder and chair of the Diversity in Nurse Anesthesia Mentorship Program (www.diversitycrna.org) and chief nurse anesthetist at Mainline Endoscopy Centers.
Martina Steed is a CRNA and Associate professor and Assistant director in the Department of Nurse Anesthesia at Webster University in St Louis, Missouri. She is also a small business owner and PhD candidate in the College of Health Sciences at Walden University.