The 57-year-old woman is standing in the hall outside of the exam room. She is agitated. “I’m waiting for the doctor. I’m freezing! My back is killing me!” I note she is pale, unable to stand still, and has a sheen of perspiration on her forehead. She is in withdrawal. I get her a blanket and ask her to wait in her room. The pain clinic nurse is downstairs at the pharmacy getting the patient’s prescription for Suboxone for induction. Induction is the process of starting the patient on medication and finetuning the dose.
An hour later the patient is back in the hall calling me, “Thanks for the blanket!” She is smiling. Her color is back. She is clear eyed, calm, and collected. What happened? Suboxone. Suboxone is a combination of buprenorphine and naloxone that is used to treat opioid addiction. Buprenorphine is a partial agonist of the μ-opioid receptor with a high affinity and low rate of dissociation from the receptor. In English, the buprenorphine molecule sticks to the opioid receptor in the brain, but only partially activates it. Then it stays there for a long time, blocking it from opioids, before dissociating. What this means for the addict is that they get enough opioid receptor activation that they don’t get sick from withdrawal. They can function normally with less of the problematic effects of a full agonist like morphine or heroine.
The addition of naloxone, a
full opioid antagonist (blocker), keeps the Suboxone pills from being crushed and injected. Though naloxone has a strong effect when given parenterally (by injection), its effect when given by mouth is negligible because it is poorly absorbed sublingually. Suboxone disintegrating tablets are given under the tongue.
So, what is this wonder drug all about? In 2000, federal legislation (Drug Addiction Treatment Act of 2000) made office-based treatment of narcotic addiction with schedule III-V drugs legal. Until then, the only option for addicts was abstinence-based treatment or methadone clinics. The ever-increasing rates of drug overdose deaths in the United States showed this was not working. At first, only MDs specially approved by the Department of Health and Human Services could prescribe medications to treat addiction. In 2016, President Obama signed the Comprehensive Addiction and Recovery Act allowing nurse practitioners and physicians assistants to prescribe schedule III-V drugs for the treatment of addiction. Previously, they could prescribe these medications to treat pain but not to treat addiction.
What does this mean for the addict? For starters, Suboxone and similar drugs are now more widely available. Until recently, the only way for a heroin addict to keep from getting withdrawal sickness was to use more heroine. These patients were considered toxic to regular doctors because their disease lead to ever-increasing doses, seeking medications from multiple providers, decreasing levels of health, and ultimately death. Now that there is an option other than going cold turkey, the addict without some kind of pain diagnosis can get access to health care whereas before they would avoid it because of the stigma of being an addict. Because Suboxone is a partial agonist with high affinity to the μ-opioid receptor, it decreases the ‘high’ if the patient continues to use narcotics causing the patient to lose interest. It offers the benefit of allowing the addict to function in life, decreases the likelihood of death from respiratory depression, and increases the quality of life because there is no need for the addict to ride the wheel of withdrawal—drug seeking, using, running out, and then seeking again to the exclusion of every joy of life.
What happens when a person starts buprenorphine? After a largish battery of tests, the prospective recovering addict will be asked to abstain from narcotics before induction to Suboxone. How long before the first dose the addict has to abstain depends on the person’s addiction. Longer acting drugs like methadone could be 24 hours. Shorter acting drugs like morphine could be as little as six hours. The person should be in the early stages of withdrawal. The reason for this is the “partial” part of partial agonist. The buprenorphine molecule will muscle other narcotics off the receptor site where it was fully activating the receptor. Now, the higher affinity buprenorphine is sitting there doing half the work that the heroine was doing and this leads to symptoms of withdrawal. Giving a person a drug that puts them immediately into withdrawal will turn them off to it completely. You won’t see that person again. Higher success rates are tied with higher levels of symptoms of withdrawal before induction. Now instead of precipitated withdrawal, the person has relief from symptoms of withdrawal even if they are not getting high.
A person who has been successfully inducted to Suboxone therapy will find almost immediate relief. The terrible body aches, muscle pain, abdominal pain, depression, diarrhea, and cravings evaporate. Our patient might just have found a new way to live, free from the constant need to find more narcotics. She can focus on her life instead of her disease. Most of the clinic patients have jobs. They want desperately to be productive members of society for themselves and for their families. Buprenorphine therapy coupled with lifestyle interventions provided by mental health professionals, self-help groups like Narcotics Anonymous, and patient-initiated interventions (like taking a class or going back to school) are part of the success story of a growing number of recovering addicts.
What’s it like to come off Suboxone? Eh, probably a lot like getting off heroine. Same withdrawal profile or pretty close. Patients wanting to get off all narcotics, including Suboxone, can be weaned off gradually depending on their desired treatment goals. Someone facing a jail sentence or travel overseas that needs to detox from opioids quickly may be on a tapered dose of Suboxone for just a few days or weeks. Other people may decide that the burden of staying on Suboxone is worth not having to go through withdrawal and choose to stay on a maintenance dose for the rest of their life. The addiction specialist will help guide the patient through the decision process. Many patients decide to stay on the medication as a hedge against relapse since buprenorphine has a higher affinity for opioid receptors than street drugs. This coupled with the very slow rate of dissociation means that a person would have to stop the buprenorphine well in advance of restarting heroine or other opioid in order to get high.
What does this mean for health care? For one, at least some addicts who eschewed health care in the past can now get treatment for this disease. At some point, most addicts will desire to get off narcotics. Having a real treatment option available instead of a far-away methadone clinic or withdrawal will work to drive these patients into recovery. Another thing is that it’s possible that some of the stigma of addiction will be lifted, at least slowly, as treatment becomes available and success stories become commonplace. As the DEA and FDA work to get a handle on the 70,000 overdose deaths per year by educating doctors and enforcing distribution laws, these drugs will become harder to get. During the 12 months prior to July 2017, overdose deaths fell in 14 states for the first time during the opioid epidemic, according to the Centers for Disease Control and Prevention. In the rest of the nation, at least the numbers have leveled off. Greater access to Narcan (brand name of naloxone, one of the drugs in Suboxone), and more treatment options for addicts will hopefully drive these numbers lower over time. It’s not time to celebrate, but at least there is a glimmer of hope. The priority is to keep addicts alive until they can (or they are ready to) get treatment for their disease.
First described by the Egyptians in 1550 BC as “sending forth heat from the bladder,” the urinary tract infection (UTI) is a frequent diagnosis seen in urgent care and doctor’s offices. Burning upon urination, urinary frequency, urinary urgency, smelly urine, and new or changed discharge—these are the hallmarks of a UTI.
Cystitis is an infection of the lower urinary tract. Pyelonephritis is an infection of the kidneys. UTIs affect about 150 million people every year with women greater than men. During any one year, about 10% of women will have a UTI and half of all women will have a UTI in their lifetime. Risk factors include sexual intercourse, diabetes, obesity, female anatomy, and family history. Although sex is a risk factor, UTI is not considered a sexually transmitted disease and a female can get a UTI even when a condom is used. E. coli is the most frequently isolated organism, though other coliform bacteria or yeast could be the culprit.
Most UTIs are caused by bacteria entering the bladder from the urethra. Bacteria then ascending the ureters into the kidneys causes pyelonephritis. Bloodborne pathogens can also lead to pyelonephritis. The urethra is shorter in women so the path to infection is shorter. Use of antibiotics can increase the risk of UTI, probably because the normal flora of the vagina or external urethra in men is disrupted. Indwelling catheterization is also a strong risk factor for UTI from organisms ascending the catheter and the normal complete emptying of the bladder is impossible due to the design of the catheter inlet opening above the balloon. It is estimated that for every day a patient is catheterized with a balloon catheter, the risk of UTI goes up 3-10%. Between the ages of 20 and 50, there is a 50-fold difference between female and male infection rates with that number decreasing over the age 50 and favoring males due to prostate enlargement, decreased bladder emptying, and increased rates of catheterization. Other risk factors are incontinence, poor hygiene, systemic disease, and hospitalization.
The gold standard of diagnosing the uncomplicated UTI is the presence of symptoms and isolation of a pathogen by culture of the urine. In reality, most uncomplicated UTIs are diagnosed clinically and with the aid of the multi-reagent urine dipstick. There are various algorithms used in diagnosis with varying levels of sensitivity (true positive) and specificity (true negative). The presence of nitrite, a product of bacterial respiration, along with leukocyte esterase and/or blood in the urine are strong indicators of a UTI and usually enough to warrant treatment with an antibiotic. For some practitioners worried about overuse of antibiotics and the resulting problems with resistance, a prescription is given with instructions not to start until the culture comes back, usually 48 hours unless symptoms progress.
Gram-negative bacteria often associated with UTIs convert the nitrate in urine to nitrite as part of cellular metabolism. This test isn’t particularly accurate because other organisms (Gram-positive) and yeasts that cause infection do not possess this trait. You can’t hang your hat on this test alone.
Leukocyte esterases are found in certain leukocytes normally associated with bacterial urinary tract infections. They are not found in normal leukocytes, epithelial cells, and bacteria of the healthy urinary tract. Certain conditions like trichomonas, chlamydia, and interstitial cystitis/nephritis can evade detection with this test so it is indicative only.
Blood in the urine can come from trauma (kidney stones) or bacterial mechanisms that lyse red blood cells and so blood can be detected either as whole blood cells or as hemoglobin, the molecule within the cell which has been spilled out by the bacteria. A dipstick positive for blood, nitrite, and leukocyte esterase in addition to one or more patient symptoms (frequency, urgency, pain, or discharge) has a high specificity for a UTI. It’s important to note that the presence of stones is also a risk factor for infection.
A complicated UTI is considered any UTI in a child, presence of a structural or functional urinary tract obstruction, recent urological surgical procedure, or a comorbidity increasing the severity of infection such as uncontrolled diabetes, chronic kidney disease, or the immunocompromised patient.
An uncomplicated UTI is usually treated with a short course of antibiotics such as nitrofurantoin, Trimethoprim/Sulfamethoxazole, or a fluoroquinolone. Some resistance is seen for all of these medications. Complicated UTIs may require longer courses or higher concentrations using the IV route. Many institutions now automatically perform a culture and sensitivity (C&S) when a urinalysis is positive. This identifies the organism (culture) and which antibiotics it is susceptible to (sensitivity).
Pyelonephritis is more serious than cystitis, sometimes necessitating hospital admission. Back pain, fever, malaise, and nausea can accompany kidney infection and this patient often looks and feels very sick. The treatment is a longer course of oral or IV antibiotics along with supportive care. The renal capsule is a tough fibrous material resistant injury. When the kidney is infected, the pressure within the organ rises and it becomes acutely sensitive. One diagnostic test for pyelonephritis is Murphy’s percussive test. One hand is placed over the costovertebral angle of the patient’s back and the other hand thumps it, causing the kidney to vibrate. Pain during this test or immediately afterwards, especially unilaterally, is highly suggestive of pyelonephritis in the patient with flank pain and fever.
If your patient is “sending forth heat from the bladder,” you should definitely do a point of care multi-reagent dipstick and send the urine off for a C&S. Flank pain, costovertebral angle tenderness, and fever should elicit a careful work up and diligent follow up.
“I feel dizzy” is a common complaint in the ER and triage nurses sometimes use the shorthand, IFD, when describing the patient’s complaint. Finding a diagnosis for this vague symptom can be challenging. One thing the nurse can do to speed up the process is to drill down to a more firm description than dizziness.
Dizziness is a complaint that can include four separate symptoms, sometimes overlapping. A careful history will reveal one or more of these: vertigo, disequilibrium, presyncope, or lightheadedness.
Vertigo
Vertigo is the feeling that the room is spinning. Often, there is a false sense of movement. Sometimes vertigo is accompanied by nausea, vomiting, sweating, and/or nystagmus. It gets worse when the patient’s head is moving. The question the nurse can ask to differentiate vertigo from other forms of dizziness is, “Do you feel like the room is spinning or moving around you?”
Vertigo has relatively few causes. Benign paroxysmal positional vertigo (BPPV), Meniere’s disease, and labyrinthitis are the most common. Less common are brain tumors, brain injury, stroke, MS, and migraines. You can see that they divide into central and peripheral causes; central causes involve the brain and peripheral causes come from the middle ear. Anything that causes inflammation in the structures surrounding the organs of balance can lead to vertigo. Often the patient will have a cold or sinus problems. Tinnitus, hearing loss, and feeling of fullness in the ear can accompany vertigo. There is a rapid compensatory process when things go wrong with the organs of balance. Usually the course is self-limiting and resolves within a few days.
BPPV is caused by loose granules of calcium carbonate moving in the semicircular canal. It can be diagnosed with the Dix-Hallpike test and can sometimes be effectively treated with repositioning movements called the Epley maneuver. BPPV does not present with hearing loss.
Meniere’s disease involves episodic vertigo along with hearing loss and a sensation of fullness, usually in one ear. There are few treatments and the disease is poorly understood. The course can last from 5-15 years before the episodes stop and the patient is left with mildly disturbed balance and decreased hearing.
Labyrinthitis is believed to be caused by a viral infection of the inner ear and can result in permanent symptoms of dizziness.
Disequilibrium
Disequilibrium exhibits itself in the patient’s gait. A stumbling or shuffling gait can be a sign of stroke, a life threatening emergency that calls for immediate activation of the emergency medical system. Other causes are Parkinson’s disease and peripheral neuropathy. Alcohol and drug intoxication frequently lead to disequilibrium. In older people, poor vision can accompany disturbances in gait, leading to falls. Benzodiazepines and tricyclic antidepressants can also lead to higher incidences of falls in the elderly.
Presyncope
Presyncope is a problem of circulation and is most commonly described as feeling like one is going to pass out without actually losing consciousness. It’s either a pump or a fluid problem and exhibits as orthostatic hypotension. When the patient stands up, he or she gets dizzy. It can be caused by dehydration (fluid problem), arrhythmias, myocardial infarction (pump problem), multiple medications, or debilitating illness. The nurse should ask the patient if he or she gets dizzy when standing up from a sitting position.
Lightheadedness
Lightheadedness is often associated with a psychiatric diagnosis and/or hyperventilation. Anxiety is the number one factor predisposing a person to lightheadedness. It is reproducible with voluntary hyperventilation.
Asking the patient a few extra questions and taking a careful history can assist the provider in making a diagnosis. Dizziness is not a very good descriptor of this problem, so drill down a little.
Nine years ago, I was so happy to have my first article published in Minority Nurse. The article was a discussion on whether or not it’s OK to be out at work as a gay person. Looking back at the changes I’ve seen over this time period, I decided to put together a few thoughts.
The county hospital where I work is rolling out some new intake questions for our electronic health record system. The impetus is to better serve our LGBTQ patients. A transgender person with residual breast tissue did not know he could still get breast cancer. A MTF person developed prostate cancer. These patients slipped through the cracks because they lived their true self but had body parts susceptible to illness that the caregiver was not aware of. By next month, we hope to have 10% of our patients properly classified using our new Sexual Orientation and Gender Identity (SOGI) questions. As the program rolls out, we will capture
more and more of our population so caregivers can better serve them.
As a gay man in my 50s, I have seen great changes in my lifetime on LGBTQ issues. There was a time when just being out was a danger. But we bring some unique perspectives to our job that shouldn’t be overlooked. We know what it’s like to be the underdog. We cherish family because we worked so hard to have our families recognized. Respect for minorities come easily to us because we have suffered discrimination. Fairness in treatment under the law was not free for us or other minorities so we always strive to protect our patients’ rights. We know that being gay does not give you AIDS, but we also know what those risk factors are and we are able to educate our patients on the facts without judgement.
Now that we are rolling out a campaign to identify our patients’ unique needs regarding sexual health, reproductive issues, and mental health, we are working to destigmatize these issues in our community. Just asking these questions can be a litmus test of our own feelings. When the program was being explained in an employee meeting, there was pushback. “Our patients will be insulted.” Or, “Our patients won’t understand the terms.”
It occurred to me that we might be projecting our own feelings and, in some cases ignorance, onto our patients. Of course, there are what seem like valid issues when trying to tease this information out of patients in the geriatric clinic. My feeling is that you just throw the questions out there and you get what you get. The elderly are just as much part of the world as the young (and in between).I can’t wait to get some real world experience in asking these questions:
What is the sex on your original birth certificate?
What is your gender identity?
What is your sexual orientation?
Some explanation might be needed with some patients. Sexual identity is not your sexual orientation. Sexual identity cannot be inferred from your birth certificate. We are looking forward to the rollout but with a bit of trepidation because we are not used to asking such personal questions. But,if you want to better serve this population, you have to identify them. The FTM person who never got a breast cancer screening because his caregivers never informed him of the risk—that can be preventable with better understanding of our patients. More information is better than less.
I take away two points from the SOGI questions that excite me. The first is that caregivers are going to be more aware of the disparities in health care that can occur with our LGBTQ patients. We are charged with the care of all our patients, not just the ones that fit into neat boxes. Just being aware of the differences makes us stop to weigh implications that might have been missed in the past. The second is that by normalizing this conversation, both patients and caregivers can talk openly about a subject that was once taboo. It’s OK to be gay or lesbian, FTM, MTF, something in between, or nothing at all. We all have health care needs.
Annette Smith, a nurse and coworker with 35 years of experience, has insight into changes in practice like the new SOGI questions: “At the beginning, there is a lot of pushback. The sky is falling, the sky is falling. But after a while, the process becomes normalized and it’s not a big deal anymore. We end up wondering what all the fuss was about!”
There was a time when just talking about sexual orientation was not even considered. Now we are required to ask! This destigmatizes the whole subject. To revisit my first question: It should never be a question of whether it’s right or wrong to be out at work. It’s just a question of you being comfortable enough in your own skin to let other people know.
A1C, or Hemoglobin A1C (HbA1c), is considered the gold standard for managing diabetes. But what is it?
The cell wall of the erythrocyte is permeable to glucose. Exposed to this glucose, the Hemoglobin molecule becomes “glycated.” The naming convention for HbA1c derives from Hemoglobin type A being separated using cation exchange chromatography. The first fraction, considered the pure Hemoglobin A is designated HbA0. After that comes HbA1a, HbA1b, and then HbA1c respective of their elution. Hemoglobin exposed to a normal level of glucose has an average glycation. As the glucose level rises, so does the fraction of glycated Hemoglobin, in a predictable way.
The average lifespan of a red blood cell is about 120 days before the cell membrane starts showing signs of wear and tear and they get shuttled off to the spleen, liver, and bone marrow for breakdown and recycling. The A1C therefore is a picture of the AVERAGE blood sugar over the previous 2-3 months. As an average, it cannot tell the difference between someone with tightly controlled blood sugar and a person with wildly fluctuating highs and lows. Neither does it identify episodes of hypoglycemia or periods of critically high blood sugar values. It’s great for population management but too crude a tool to manage an individual patient.
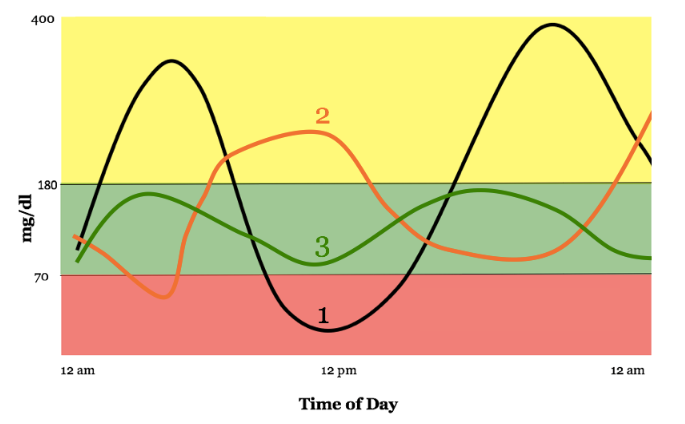
In the chart, we see a day in the blood sugar levels of three patients. All three have the same average blood sugar, but patient number 1 and patient number 2 have wildly fluctuating levels throughout the day. Patient 1 spends more time outside of range than inside, but her A1C would be normal.
The A1C coupled with the patient’s daily blood sugar record gives a more complete picture for individual patient management. Other shortcomings in the A1C happen with patients with high or low blood cell turnover. Patients with kidney disease undergoing dialysis have especially high turnover of red blood cells due to the process of filtering the blood. Their A1C would be abnormally low. Cirrhosis of the liver decreases blood cell turnover leading to higher A1C levels. Certain types of anemia and blood disorders as well as some vitamins and medications can affect the accuracy of the A1C. If you hang your hat on the A1C for all your treatment decisions, you will be misled.
So, what is the A1C good for? The American Diabetes Association has the following guidelines to be used in the diagnosis of diabetes:
A1c Level
What It Means
Less than 5.7%
Normal (minimal risk for type 2 diabetes)
5.7% to 6.4%
“Prediabetes,” meaning at risk for developing type 2 diabetes
6.5% or greater
Diagnosed diabetes
Following it over time allows for risk evaluation for complications arising from diabetes. There’s a strong positive correlation between high A1C numbers and diabetic neuropathy, kidney disease, and eye disease. Diabetic specialists use the daily blood sugar levels to formulate an individual plan for each patient to drive the A1C numbers lower over time.
Understanding the A1C and what it does and does not tell you is important. It’s a great starting point, but not an accurate tool for individualized diabetes care.