For 15 years, Latanya Weston was in operating rooms in her home state of Georgia, amputating the limbs of patients who suffered from kidney disease. The feeling of the scalpel pushing down on flesh and the sound of the bone cracking haunts her.
A Georgia native, Weston knew that the mortality rate of kidney disease is 30 to 40 percent higher in her state than the national average. But, while the numbers show that the percentage of black and white adults treated for kidney disease are roughly the same, Weston knows a different reality.
The series highlights healthcare leaders who are prominent figures in their organizations and are making transformational impacts in nursing.
Meet Latanya Weston, a nurse practitioner at Somatus, the nation’s leading and largest value-based kidney care company.
Talk about your career path and how you ascended to that role.
I was constantly stricken with various illnesses when I was growing up. As a high school student, I spent most of my senior year being operated on or hospitalized. Although I could maintain my overall academic achievements through these health issues, I was told I would need to repeat my first semester as I had been in the hospital too much. It was unfair to the other students. This news was incredibly disheartening. I had already mapped out a career plan and did not want to delay graduating. I made a tough decision and begged my parents to let me sit for the “General Education Development” exam. I excelled and went on to sit for the SATs. I became a college student while my friends were still in high school.
Once graduating from the surgical technology program, my career path began at Mitchell County Hospital, where I was a surgical technologist. Together our surgical team operated on many patients suffering from advanced kidney disease and renal failure. In many cases, these patients had developed peripheral arterial disease. They were on the table to have a limb amputated or were crashing into dialysis and needed to get a venous catheter implanted. Although I loved being a surgical technologist, my heart’s desire was always to become a nurse. So, in 2006, while working as a surgical technologist, I returned to school and became an operating room nurse. This allowed me to work at a bigger hospital in my hometown to gain more experience. However, the unsettling patient trends I had noticed in the county hospital were now amplified—more amputations and dialysis catheters, and again always in patients of color. So, in 2007, I again shifted my career and decided to leave my hometown for a hospital away from home.
After more than a decade along this career path and seeing patients in severe distress day after day, I grew to feel I needed to make a change. Then, one day while I was on call for the operating room, I fell down a flight of stairs and hurt my foot. The pain was constant, and I could no longer stand on my feet in the operating room as long as I had. I had to make a change, and a part of me felt like this was a sign that I should go back to school to educate and prevent the disease processes that were landing so many patients on the operating room table. For quite a while, I had been thinking about what impact I could make if I met patients earlier in their healthcare journey before surgery was the only option. I then decided that I would become a nurse practitioner.
What inspired you to become a nurse?
I knew I wanted to be a nurse from a very young age. My aunt was a nurse who would conduct home health visits at her patients’ houses, and from the time I was in second grade, I would beg to go with her. I enjoyed visiting patients and watching my aunt care for them. I always felt I had this same gift of caring as she did. Nursing takes a special heart and mind; everyone does not possess this attribute.
Furthermore, I grew up in a community with significant health challenges, yet people didn’t prioritize their health. Most people don’t have primary care physicians, schedule annual check-ups, or think about preventive care. Members of my community were often struggling with obesity, diabetes, and kidney disease, and there were several dialysis centers in my neighborhood. Kidney disease impacted my family as well. My sister passed away at 33 because she could not get a kidney transplant.
I’ve lived my whole life in Georgia, where the mortality rate from chronic kidney disease is over 40% more than the national average.
As a nurse practitioner, I finally feel I am where I was meant to be. Now I reach patients early on in their healthcare journey when their primary care physician first diagnoses them with kidney disease. Through education and support, I can change the direction of a person’s life and stop them from ending up on someone’s operating room table.
What are the most important attributes of today’s nursing leaders?
Given the changes in the healthcare industry, building trusting relationships between clinicians and consumers can often be taxing. Nursing leaders must be of great character and moral values. This includes the ability to show respect to another and communicate appropriately. One of the major complaints in the patient population is that providers do not listen. As nursing leaders, we can’t overstate the importance of being a good listener and communicating relevant information to providers. This will strengthen the patient-provider relationship and encourage more communication, improving overall patient outcomes. Nurse leaders must maintain integrity, respect, grace, and professionalism and always take the time to listen and communicate, making their relationships the building blocks to success.
What does it mean to you to be a nursing leader, and how are you making a difference?
The leader I am today is the ultimate assignment. I wanted to uncover the world of medicine and was given the great opportunity to travel as a Locum Tenens Nurse Practitioner from 2016 to 2018. That experience blessed my entire being and made me realize that my mission is not only to save lives but to change them. I worked in the Pacific Northwest to combat mental illness and addiction and changed many lives. In every home or exam room I enter, the person on the other side of the door becomes my family. No matter the situation, I take their hands, and together we weather the storm one diagnosis at a time. I ensure they do not feel alone in the battle, which makes a difference in patient outcomes.
What is the most significant challenge facing nursing today?
The healthcare industry has come a long way in recognizing the impact of social determinants of health on patient health, but this is still the most significant challenge facing us today. As nurses, we see first-hand, time and again, that providing “equal” care to patients is not enough. Care plans must consider the whole person, where they live, their resources, and everything else that affects them when they leave their doctor’s office.
This is particularly true about kidney disease, which disproportionately affects Black people. Black people make up around 13% of the U.S. population but account for around a third of those with kidney failure.
In many cases, patients don’t realize they have kidney disease until the day their doctor gives them the diagnosis. Without understanding the disease process and how each element of the care plan works together to slow and control their chronic kidney disease progression, it’s very difficult for a patient to commit to making significant lifestyle changes.
We also know that socioeconomic issues are tied to kidney disease. Even if a patient has health insurance, they may still have financial concerns, making it difficult to afford medications and treatments. They may be worried about paying their rent or utility bills, which makes it difficult to focus on their physical health. In addition, they may not have a wheelchair or a ramp to get in and out of their house or transportation to their next doctor’s visit.
Shopping for kidney-friendly foods may also be a challenge, both in terms of affordability and availability. Patients may also need help adopting new meal preparation methods with no one to guide them, and they find it much easier to fall back on frozen meals.
There are countless other barriers to care that we see in our patients every day, and as nurses, we are often the best equipped to inform the rest of the care team about what our patients need.
As a nursing leader, how are you working to overcome this challenge?
I’m now a nurse practitioner at Somatus, the country’s first value-based kidney care company. Our goal is to give whole-person, 360-degree support to kidney disease patients, providing preventive care and breaking down the barriers and challenges patients face every day. For example, when a patient is first diagnosed with kidney disease, we go to the patient’s home to do a complete evaluation, look through their cupboards, figure out where they can source nutritious food, demonstrate how to prepare meals, and even help them with administrative tasks and paperwork.
Together with my fellow Somatus care team colleagues, we work with a nephrologist and other health care providers to give patients the whole-person support they need to follow their care plan and make lifestyle changes.
Every day I see the impact of individualized, patient-centered care. Sometimes there are significant actions like teaching a patient to monitor their blood pressure every day, but other times it’s something small, like praying with one of my patients, that makes a huge difference. This is what I love.
What nursing leader inspires you the most and why?
Mary Eliza Mahoney is the first African American licensed nurse in the U.S., and when I think of her perseverance and tenacity, I also see myself. She worked tirelessly as a private home nurse, doing what she loved while advocating to be treated as a professional and equal. Her example shows that we can not only prolong and save lives but can also change them.
What inspirational message would you like to share with the next generation of nurses?
When you become a nurse, whenever you walk through the door, someone on the other side waits for you to enter the room and be their guiding light. So I like to take a moment to ask myself, “I wonder who my next blessing is in that room?” every time I meet a new patient. This road is not for the weak, but the journey is incredibly rewarding as you touch and change lives day after day. I always tell people, “Nursing is not a money thing… it is a heart thing.”
The fundamental mission of every healthcare provider is to first do no harm. Unfortunately, however, for far too long systemic inequities in the healthcare system have perpetrated and perpetuated harm.
Both implicit and explicit biases have strongly determined healthcare processes, including informing how patient pain is understood, diagnosed, and treated. Stereotypes relating to gender, race, and ethnicity have contributed to a pattern of delayed and erroneous diagnosis and inappropriate or insufficient palliative care. And as a result, untold numbers of female and minority patients have been consigned to suffer needlessly.
But there is hope, and nurses are helping to provide it. By prioritizing workforce diversity, qualified healthcare professionals enjoy greater career opportunities, and diverse patients increasingly receive the pain control they need. This article examines the importance of diversity in the healthcare industry and its implications for improving palliative care for diverse patients.
Biases and the Treatment of Pain
Generally, healthcare providers enter the field because they genuinely want to help people. Of course, financial security and social prestige are a perk, but no matter your particular role, the work is incredibly emotionally, cognitively, and physically demanding. Nevertheless, it is a profession you enter or remain in with a sense of a higher calling and a deeper purpose.
But, no matter how well-intentioned, healthcare providers are still very much human, and as such, they are shaped, both consciously and unconsciously, by the society in which they live. And that means that systemic biases have almost inevitably seeped into the care provider’s consciousness, contributing to the formation of false and dangerous stereotypes.
Research has shown, for example, that racial stereotypes concerning African-Americans have contributed strongly to the mismanagement of Black patients’ pain. These stereotypes are generally rooted in misperceptions of biological differences between African-American and Caucasian patients. This includes the false belief that Black patients have a higher pain tolerance than whites and the false presumption that Black patients are more likely to abuse drugs.
Implicit and explicit gender biases are also ubiquitous in modern medical practice. For example, female patients complaining of pain are more likely to experience treatment delays than male patients reporting the same or similar symptoms. Women’s pain symptoms, for instance, are significantly more likely to be attributed to emotional or psychological etiologies than men’s. This increases the likelihood that their pain will go untreated or under-treated, and severe disease symptoms will go unrecognized, thus delaying treatment.
Diversity and Cultural Competence in Healthcare
Nurses are at the front lines of patient care. They provide the majority of hands-on patient care, and, in general, their interactions with patients are more frequent and substantive than those of physicians.
For this reason, diversity in the nursing sector is particularly critical in redressing inequities in treating patients’ pain. Culturally competent patient care almost inevitably ensures that nurses derive from various ethnic, racial, socioeconomic, and gender backgrounds.
More specifically, this means that nurses with high cultural competence will better understand, recognize, and respond to culturally-specific manifestations of patient pain.
For instance, women or patients from specific cultural or religious backgrounds may feel reluctant or unable to express their symptoms, especially if these pertain to “taboo” areas. Nurses from similar backgrounds are more likely to have the cultural competence to identify and overcome these cultural taboos.
This enables them to formulate strategies that help patients express their concerns in more comfortable and culturally acceptable ways. In addition, by enhancing the dialogue with patients, nurses can provide physicians with more comprehensive and accurate case notes, increasing treatment efficacy.
Addressing Medical Anxiety
Promoting diversity in nursing doesn’t just equip healthcare teams to understand and address cultural differences among patient populations effectively. Diversity also enables healthcare teams to recognize and remediate systemic healthcare disparities’ profound and long-enduring impacts.
There is mounting evidence, for example, that minority patients are far less likely than Caucasians to be satisfied with their quality of medical care. Deficiencies in minority patient care can be linked to various factors, from the lack of healthcare access to a shortage of interpreters for patients who do not speak English.
These care deficiencies can instigate severe medical anxiety in patients, particularly for those who have experienced significant physical or emotional trauma in past medical encounters. Nurses from similar backgrounds may have also experienced such challenges in the healthcare system, whether for themselves or someone they love. And as such, they are more likely to be able to accurately anticipate or ascertain signs of medical anxiety in female and minority patients.
Equipped with such insight, diverse nurses can lend a measure of patient support and empathy that comes from understanding and experience. And, importantly, they can more effectively advocate for patients and their unique needs, particularly in treating pain.
The Takeaway
Disparities in the healthcare system have for too long led to deficiencies in palliative care for minority and female patients. By promoting diversity in the nursing profession, however, the needless suffering to which diverse patients have been subjected can finally end.
For more than a century, nursing has been thought of as the domain of women. But that has fluctuated over the last few centuries. Men actually dominated nursing through the mid-19th century. During the Industrial Revolution, men began leaving nursing for factory jobs. Florence Nightingale led the advancement of women in nursing, targeting upper and middle class women for nurse training. In fact, men were not allowed to serve in the Army Nurse Corps during World Wars I and II. Today, as workplaces evolve, more men are entering the profession again amidst a nursing shortage.
Entering Nursing
About 13% of nurses in the U.S. today are men, compared with 2% in 1960, according to the Washington Center for Equitable Growth. However, in the high-paying specialty of nurse anesthetist, there is an equal number of men and women.
The United States is leading the way in the increase in the number of male nurses. While the U.S. rate of men in nursing was not much higher than in Switzerland and Brazil in 1970, it rose rapidly over the next several decades and far surpassed these countries in addition to Portugal and Puerto Rico.
The rise of men in nursing is due in part to a shift in available jobs, especially as traditionally male-dominated jobs in manufacturing jobs like automakers have been taken over by automation or moved overseas for cheaper labor. A recent study published in the journal Social Science Researchreviewed eight years of Census data. The study found that of men who had worked in male-dominated industries and then became unemployed, 14% decided to enter industries dominated by women, such as nursing. Eighty-four percent of men who didn’t lose jobs moved onto traditionally female jobs. Unemployed men who got jobs in female industries received a pay increase of 3.80% when making the move.
Where the Jobs Are
Another reason propelling more men into nursing is a shortage of nurses. According to the Bureau of Labor Statistics (BLS), employment for registered nurses will grow 12% between 2018 and 2028, much quicker than the average of other professions. There will be a need for 3.19 million nurses by 2024.
California is expected to have the highest shortage of nurses, and Alaska will have the most job vacancies. Other states that will face shortages of nurses in the next few years include Texas, New Jersey, South Carolina, Georgia, and South Dakota.
One driver of the need for more nurses is the growth of the aging population, who will require more medical care. Job growth is expected in long-term care facilities, especially for the care of stroke and Alzheimer’s patients. The need for nurses treating patients at home or in retirement communities will continue to grow. The rise in chronic conditions such as diabetes and obesity also means more nurses will be needed.
Pay and Training
The median annual wage for registered nurses was $71,730 in 2018, according to the BLS. The lowest 10% earned less than $50,800, and the highest 10% earned more than $106,530. Those working for the government and hospitals earned the most.
But like many other professions, men are outpacing women in pay. Male RNs make an average of $5,000 more per year than their female counterparts, according to a study published in the Journal of the American Medical Association. This salary gap hasn’t improved since the first year the salary survey was done in 1988. The difference in pay ranges from $7,678 per year for ambulatory care to $3,873 for work in hospitals. The largest gap, $17,290 for nurse anesthetists, may explain why so many men enter that specialty.
The researchers note that increasing transparency in how much employees are paid could help narrow the gap. In addition, part of the pay gap may be due to women taking more time out of the workforce for raising their children. FiscalTiger.com suggests that offering adequate leave to both mothers and fathers after the birth of a child could have a role in making pay more equitable.
The Washington Center for Equitable Growth’s report suggests that the amount of formal training required to become a registered nurse may bring men into nursing from other occupations later in their careers. The minimum training for registered nurses is an Associate Degree in Nursing. Increasingly, employers are demanding more education, however. That includes earning a Bachelor of Science in Nursing (BSN) degree. RNs in the U.S. military must have a BSN, and the Veteran’s Administration, which employs the most RNs in the country, requires a BSN for promotion.
Finding Support
While men are still a minority in nursing, various programs offer support and networking. The American Association for Men in Nursing was founded in 1971 but shuttered in a few years. In 1980 it was reformed and now has thousands of members. It encourages men of all ages to become nurses and supports their professional growth.
Some nursing schools also have groups to support male nursing students. New York University, for example, has Men Entering Nursing (MEN), open to all nursing students at the Rory Meyers College of Nursing to discuss the concerns and perceptions that affect men and what it means to be a male in the field of nursing.
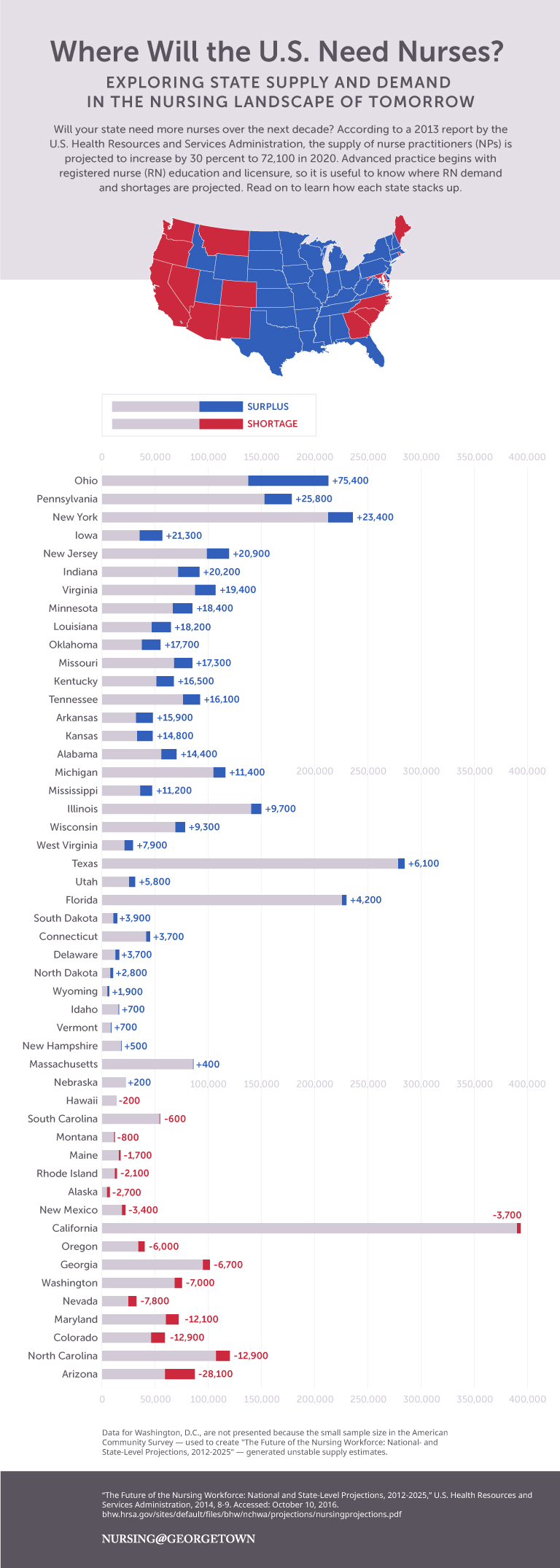
Nurses make up the largest segment of the health care workforce in the United States. There are more than 3.1 million registered nurses nationwide and about 85% of these RNs are employed in nursing. Yet, some states are predicted to experience a nursing shortage during the next decade as the result of changes in health care policy, an aging population, and nursing schools struggling to make space for more students.
A report from the Georgetown University Center on Education and the Workforce titled, “Nursing: Supply and Demand Through 2020,” predicts a shortage of approximately 193,000 professional nurses by 2020 based on the age of the current nursing workforce, the size of graduating nursing classes, and nurses’ career decisions. A 2012 report titled, “United States Registered Nurse Workforce Report Card and Shortage Forecast,” concurs. It predicts a nursing shortage by 2030 throughout the country, especially in the West and South, because of projected changes in population.
Nursing@Georgetown’s online FNP program created the graphic below based on data from a 2014 HRSA report, “The Future of the Nursing Workforce: National- and State-Level Projections, 2012-2025,” to show which states will have a shortage of nurses and which will have a surplus.
To learn more about the nursing landscape, visit Nursing@Georgetown’s website to read the original blog post.
The University of Florida (UF) College of Nursing has named Dr. Jeanne-Marie Stacciarini, PhD, RN, FAAN, its first director of diversity and inclusion. Created to enhance awareness and dialogue about important issues in diversity, the newly established position was created based on recommendations from UF’s diversity and inclusion task force.
Stacciarini is an associate professor in the college and has been with UF since 2006. Her research focuses on mental health promotion among minorities and community-based participatory research for minority, rural, and international populations. Stacciarini has been recognized for her work with underserved populations with the 2012 Southern Nursing Research Society (SNRS) Award for Research in Minority Health and the 2014 APNA Award for Excellence in Research. Outside the College of Nursing, Stacciarini is a leader on campus as chair of the UF President’s Council on Diversity and she sits on President Fuchs’ leadership cabinet.
In her new position she aims to create better dialogue and educate others about the need for diversity. She will work on student and faculty recruitment to create a better working and learning environment. Leading a new initiative with undergraduate students in the College of Nursing, Stacciarini will be launching a program called Engaging Multiple-communities of BSN students in Research and Academic Curricular Experiences (EMBRACE).
UF College of Nursing Dean, Anna M. McDaniel, says she believes that Dr. Stacciarini’s diversity work will have a positive impact on the entire college and serve as a campus-wide model. Dr. Stacciarini is a tireless advocate for faculty, staff, students, and patients from diverse and underrepresented backgrounds, and as director of diversity and inclusion she will play a lead role in carrying out the College of Nursing’s commitment to diversity and inclusion for all members of the community.
Casey Dillon, a nursing graduate student in the college and former student of Stacciarini says she thinks more diversity in the college will prepare students for nursing careers. Nurses work with a wide variety of people every day, so diversity education is a necessary thing.
As nurses, Stacciarini says we need to be prepared to care for a more diverse patient body. She is honored to fill this important position and work to help more people understand diversity and inclusion to sustain that culture across the College. She hopes to bring ideas from the President’s Council on Diversity to new initiatives in the College of Nursing.