It is certainly no secret that American Indians suffer disproportionately from many serious health problems, including diabetes, cancer, AIDS and substance abuse. Nor is it news to most nursing professionals that more research into the causes of these health disparities is urgently needed in order to develop effective, culturally competent prevention and treatment programs. But despite this common knowledge, American Indian populations and their culture are familiar yet foreign to much of the nation’s nursing community.
Because Indians are severely underrepresented among the ranks of nurse scientists, many non-Indian nurses have conducted research in Indian communities–or have attempted to do so. The key factor in determining whether such research projects will be successful or fruitless is the nurse’s awareness of, and ability to overcome, the unique challenges involved in working with Indian populations. Many of these challenges relate specifically to the issue of conducting research in a manner that is culturally sensitive to Indian communities’ needs.
The first challenge researchers must meet is that of establishing trust and proving their commitment to conducting research in a culturally respectful way. Many Indian tribes are distrustful of outsiders and do not welcome researchers into their communities. Furthermore, Indian communities have been the focus of hundreds of research studies over the years but have not always had the opportunity to benefit from these projects and their findings. Because of this overuse of Indian communities, many tribes have become closed to non-Indian researchers.
Nurse researchers need to understand that it takes time to build trust. Sometimes, getting a research project started in a tribal community can take one to two years–or more–of preparation before the researcher can even begin the study. Therefore, researchers not only need to be committed to overcoming barriers of distrust but must also be willing to commit time to getting access to the Indian community.
Getting It Right
There are several culturally sensitive steps a researcher can take when preparing to conduct a study in an American Indian community. The first step is to identify what type of Indian community it is–a reservation, a non-reservation community, an Indian nation, a tribe, a band, a federally or non-federally recognized tribe or an urban community.
This knowledge is important because there are cultural and historical differences between these various types of communities, such as languages, degrees of assimilation, means of identifying tribal members, and sustained cultural practices, to name a few. There are also differences in community size, tribal governance and the tribe’s relationship with the U.S. government. Researchers must be familiar with these distinctions in order to address the community and its members knowledgeably and appropriately.
For example, an Indian reservation is a self-contained tribal entity with its own government, governing rules and land base, while a non-reservation Indian community–such as those in Oklahoma–may have a tribal government but not the land base. The terms “Indian nation” and “tribal nation” refer to the largest Indian communities, while “band” usually refers to smaller groups of people within one tribe–e.g., the Ojibwe tribe has many bands, and the governing structure for each band may vary. Therefore, members of an Indian nation may be offended if an outsider calls it a band or a tribe, and vice versa.
Researchers also need to consider the region of the U.S. in which the Indian community is located–e.g., Southwestern, Southeastern, Northwestern, Eastern, state of Oklahoma or state of Arizona. Each region has had its own impact on the history and development of the Indian communities it contains.
For example, in Oklahoma during the territorial days, the state was made up of many Indian reservations. But in the early 1900s these reservations were taken away from the tribes, and each enrolled Indian person was instead given a parcel of land. This change in the land base dramatically altered the way of life for Oklahoma Indians.
In addition to learning as much as possible about an Indian community’s history, structure and culture in advance, a researcher preparing to conduct a study in that community may also want to visit the area. Much can be learned from visiting the community’s cultural center, attending a public Indian event in the community, visiting a historical Indian site, talking to the local Indian people and becoming familiar with the local customs.
When visiting the Indian people, a researcher who is culturally sensitive will ask them how they prefer to be addressed and how they want to be identified. For example, members of the Navajo Nation may prefer being identified as “Diné” rather than “Navajo.”
It’s also important to let the Indian people reveal information about their community in their own way and in their own time. If you ask them direct questions, you might not get answers. Indian people believe in developing a oneness of spirit with another person before information can be exchanged.
Working With What You’ve Got
Another challenge a researcher may need to overcome is the limited availability of resources in an Indian community. Because many tribal communities are poor and do not have economic development, the people who live there generally lack financial resources as well as adequate housing, transportation, sanitation, clothing or food.
Furthermore, many Indian communities are located in remote and rural areas of the country where access to necessary resources and services is severely limited. In the Deep South, for example, there are many small Indian communities in rural areas where there is no public transportation and no emergency services, hospitals, clinics, or physicians nearby to care for the Indian people. These people must drive long distances to receive health care–if they even have a car.
When conducting a research study, these kinds of factors can influence the outcome of the project. For instance, the Indian people may not even be able to arrange transportation to participate in the study. You will have to bring the study to them.
Difficulty in obtaining a large enough sample size is still another obstacle that can prove frustrating for nurses who want to conduct research studies in an Indian community. The largest tribe in the U.S. is the Navajo Nation, which has over 250,000 enrolled members, followed by the Cherokee Nation with around 222,000 enrolled members. Most tribes, however, are much smaller in size, averaging only a few hundred or thousand tribal members. As a result, American Indians are often not included in studies examining significant health problems like breast cancer and lupus, because the sample size is too small to be statistically valid.
It is not always easy to find a solution to this problem. Some experts suggest grouping several small tribes together to increase the sample size, while others argue that this method is not always culturally appropriate and that tribes do not like to be “lumped” together in this way. Another possible approach would be to explain the reason for the small sample size and adjust the statistical significance accordingly. For example, if 50% of the people in a tribe are diabetic, this is a significant finding even if there are only 250 tribal members.
Creating Co-Ownership
Because of the negative research experiences they have had in the past, many Indian communities are now demanding more respect from outside researchers, as well as a greater sense of co-ownership in the study before, during and after it is conducted. To be culturally sensitive, nurse researchers must strive to develop a more “equal” partnership with the tribe.
[ads:other]
Traditionally, many researchers have only wanted tribal communities to assist with recruitment of subjects and nothing else. Once the data was collected, the researchers never returned or followed up with reporting the findings back to the community. The tribes did not know the outcomes of the studies. The researcher benefited from the study while the tribe received few, if any, benefits from its members’ participation in the project.
Tribes are also raising questions about who owns the data from a research study conducted in their community and are demanding more control over how the data is handled. In some studies, the findings were not only published without any input from the tribal community but also published in a way that reflected negatively on the tribe.
To cite just one example, a researcher who conducted a study on health problems occurring in an Indian community in the Midwest did an interview with a local newspaper about her findings. She did not get an opportunity to review the reporter’s article before it was printed. When the article appeared, it contained disparaging and factually inaccurate comments about the tribe’s cultural traditions and how they allegedly contributed to the Indians’ health problems.
In addition, much of the research that has been conducted with Indian populations has tended to put too much emphasis on the “culture of poverty” in tribal communities. By focusing on the effects of poverty on Indian peoples’ way of life, many researchers have overlooked the strengths of the Indian community. As a result, a growing number of tribes are insisting that researchers focus on tribal and cultural strengths instead of on health deficits.
For instance, many studies have been conducted about the breakdown of American Indian families but very few have explored the positive aspects of Indian family life. One notable exception was a recent study on Indian parenting in which the researcher described how Indian mothers parented in such a way that the harmony (natural development) of their children’s lives was promoted through passive forbearance (the Indian pattern of care).
The Indian mothers did not parent in a way that controlled their children’s development but rather in a way that enhanced natural development through unobtrusive, respectful behaviors like listening, observing and being an example to others. In other words, the researcher chose to focus on the cultural patterns of parenting instead of on how poverty impacted the parenting.
Because of these kinds of experiences, tribes that participate in research studies want more of a say into the interpretation and dissemination of the findings. A researcher may need to include the tribe in the analysis of the data and get tribal approval for publication of the findings. This kind of tribal involvement can be written into the research proposal.
Finally, many Indian communities have become more “research-savvy” in order to better protect their interests. Many tribes now have their own Institutional Review Boards (IRBs) to which potential researchers must submit their proposals. Nurses who wish to do research in a particular Indian community need to become familiar with the appropriate procedure for obtaining the tribe’s permission to conduct the project. You may need to not only get the tribal IRB’s approval for human subjects but also get approval from either the tribal chief or tribal council.
In one research study conducted with a Southwestern tribe, the researcher had to first get approval from two tribal subcommittees and then go before the 15-member tribal council before approval for the project was given. The entire approval process required five visits with the tribe, and it took six months before the final decision was made.
Sometimes tribes will “barter” with researchers to ensure that both sides benefit equally from the partnership. For example, members of one small tribe in the Deep South successfully negotiated an arrangement in which the researcher agreed to assist them in writing an economic development grant in exchange for their participation in the study.
Playing by the (Cultural) Rules
In summary, nurse researchers must remember two important ethical principles when conducting studies in American Indian communities. The first is right to informed consent. The tribe needs to know the purpose of the research, who will benefit from the research, and how the research will be conducted with appropriate tribal input.
The second principle is do no harm. The researcher has an ethical duty to protect the tribal community by not violating cultural norms, by not publishing findings without approval from the tribe and by taking measures to protect the Indians’ culture. By following these rules of cultural sensitivity and respect, nurse scientists will greatly increase their chances of successfully overcoming the challenges of conducting much-needed research on American Indian health disparities.
Being a nurse has been a calling for Mattiedna Johnson, RN, MTMA Div., of Cleveland, Ohio. In fact, it could be said that her pioneering work in health care is part of a divine agreement. The fifth child born to Arkansas sharecroppers, she tells the story of how her father, upon seeing how tiny she was at birth, begged God to spare her life. In exchange, he promised to return his daughter to God in life. As part of the bargain, Johnson’s father told her when she was just a child that she was to become a medical missionary in Africa.
Out of her determination to fulfill her father’s promise, Johnson has spent a lifetime making groundbreaking contributions to the health care field. Her work has improved both patient care procedures and the profession of nursing. She has helped form organizations for African-American nurses, been a pioneer in setting up public blood pressure screenings and conducted history-making research that helped develop a cure for scarlet fever.
These contributions have not gone unnoticed. On October 23, 1990, the Hon. Louis Stokes, one of the nation’s most prominent black Congressmen, saluted Johnson in a speech before the U.S. House of Representatives. Citing Johnson for her many accomplishments, Stokes called her “a great pioneer and a source of inspiration to our community and the nation.”
Making a Lasting Impression
Growing up in Arkansas, Johnson always knew she would one day be a nurse. As a student, she excelled in her classes. In college, she spent her weekends cleaning other people’s houses to help pay for her nursing studies.
“A Salute to a Nursing Pioneer”—The Hon. Louis Stokes on Mattiedna Johnson, RNThe following comments are excerpts from a speech made by Rep. Stokes before the U.S. House of Representatives on October 23, 1990:
Mr. Stokes: Mr. Speaker, I rise today to pay tribute to Mattiedna Johnson, RN, MA Divinity, MT, who is being honored at an upcoming “Salute to Nursing Pioneers Program.” On November 11, 1990, friends and colleagues will gather at Cory United Methodist Church in Cleveland to pay tribute to Mattiedna Johnson for her 50 years of nursing service to the community. I am pleased to salute Nurse Johnson on this special occasion and I am proud to share with my colleagues some of the highlights of her distinguished career. . .
In 1944, Nurse Johnson conducted research at the University of Minnesota Department of Plant Pathology, which resulted in the cure for scarlet fever. In 1945, she was certified by the American Red Cross and began teaching disaster nursing and basic first aid. One year later, Nurse Johnson was certified as a medical missionary and served in Liberia, West Africa, where she promoted the organization of the Liberian National Nursing Association.
Nurse Johnson moved to Cleveland in 1959, where she tutored nurses for the Ohio Board of Nurse Education and Registration, and spent much of her time as a leading American Red Cross volunteer instructor. Classes included “Mother’s Helper,” “Teenage Babysitting” and “Home Nursing.” She also developed special courses for church nurses, utilizing church basements throughout Cleveland for her classroom.
Mr. Speaker, Mattiedna Johnson has also been an outspoken and courageous advocate on behalf of black nurses. At a nurses’ convention in 1970, she called black nurses together. That meeting led to the formation of the National Black Nurses Association. She went on to organize the Cleveland Council of Black Nurses and, in 1973, with the Akron Black Nurses, she convened the first institute and conference of the National Black Nurses Association.
Although now disabled, Mattiedna has not lessened in her efforts. She is an active participant in the 21st Congressional District Caucus and the Congressional Black Caucus Health Braintrust, which I chair. In addition, she is the author of The Penicillin Project Diary Notes and is now publishing the Johnson’s Manual for Church Nurses.
Mr. Speaker, I take pride in congratulating Mattiedna Johnson. She is a great pioneer and a source of inspiration to our community and the nation.
Source: Congressional Record
In her last year of high school Johnson and another student tied for top honors in her class. Because Johnson had not been an original member of the graduating class (she skipped eighth grade), she was named salutatorian instead of valedictorian. But she was determined to prove that second place didn’t mean second best. Johnson recalls the effect her speech had on the audience attending the commencement ceremony.
“As I spoke, people stood up and listened,” she says. “They didn’t stay in their seats. When I finished my speech, they stood there and clapped for a good three minutes. Everybody was crying, although I didn’t know why. My subject was about being prepared for better things.”
In fact, her words made such an impression on those attending that even after Johnson went away to college, people in her hometown continued to remember her and her plans to be a nurse. “When I went to nursing school and came back home to visit, these people would send me a dollar and write to me,” Johnson recalls. “It was a community type of thing, a small town thing.”
Johnson graduated from Jane Terrell Memorial Hospital School of Nursing in Memphis, Tenn., in 1940. She then worked as a post-graduate nurse at Homer G. Phillips Hospital in St. Louis, Mo., where she earned her license as a registered nurse.
“This was a hospital where a woman had started a program to pull in nurses from small hospitals to replace nurses who had gone on to Fort Wachuca in Arizona in the U.S. Army [during World War II],” Johnson recalls.
This experience laid the groundwork for what would later become one of Johnson’s most significant contributions to health care.
“As post-graduate nurses, we could go to other programs,” she says. “I went to the St. Louis Isolation Hospital for a period of study. There I took care of a little baby, 18 months old, who had scarlet fever. His grandmother had given him some kerosene on sugar, which was the common treatment at the time. In those days, the disease was incurable. He died in my arms. When I put him in the morgue, I noticed they put a blood-red tag on his foot, a burnt-orange tag on the coffin and a white tag on the casket.”
Johnson returned to Homer G. Phillips Hospital where, one day, she saw in a physician’s magazine an advertisement for the Northwest Institute of Medical Technology in Minneapolis. She applied for the program and was accepted. On January 1, 1943, she took the train to Minneapolis, where her life would change in many ways.
“I stayed in the home of Dr. and Mrs. Winston,” Johnson remembers. “He was a professor at the University of Minnesota and his wife worked with the Red Cross. Knowing I was a nurse, she would talk to me.
“One day, Mrs. Winston was making some notes and she asked me what I would do [as a nurse] if Minneapolis were bombed and I saw someone injured in the street. I told her I would first see if the person were breathing and establish the breathing process, then I would check for bleeding. Mrs. Winston put that information in her notes and started a disaster nursing program for the Red Cross. Before she left to go to France [during the war], she gave me a Red Cross pin.”
In December, after a year of study, Johnson completed the medical technology program. In order to remain in Minneapolis, she rented rooms in people’s homes and returned to cleaning houses to pay for her expenses. One home where she lived was that of the family of her future husband.
Breaking the Mold
Not long after completing her medical technology courses, Johnson came across the career opportunity of a lifetime.
“In February 1944, there was a big article in the paper describing the U.S. Army Medical Corps’ Penicillin Project that was being brought to the University of Minnesota’s Department of Plant Pathology,” Johnson says. “I caught the early bus the next day and went to the university.” She was hired by the project’s director, Dr. Clyde Christianson, and worked on the research team for the next several months. She was the only African American, the only laboratory technician and the only registered nurse on the project.
Johnson’s experience from the isolation hospital in St. Louis helped her convince the project’s leaders of her potential value to the team. “When I first got to the university,” she relates, “I went up some steps and went into the agriculture building. Dr. Christianson was squatting down looking at some laboratory specimens. Some of them had burnt-orange tags. I told him that somewhere among the ones with the burnt-orange tags was a blood-red tag because somebody had died, which meant these specimens were contaminated. He stood up, looked at me and said, ‘What do you suggest?’”
British scientist Alexander Fleming had discovered penicillin in 1928, after observing that a common bread mold had the ability to kill bacteria that caused disease. He had been searching for a chemical that would combat many of the deadly diseases soldiers suffered in World War I. When World War II began, there was a renewed need for such a medicine.
[ads:education]
Johnson’s experiences growing up on a farm proved to have an unexpected benefit on her ability to understand and work with penicillin molds. As a child, she had been taught to churn butter and make lye soap, and she had helped her mother make apple jelly. Now, working in a makeshift laboratory in the corner of the agriculture building, she drew upon her knowledge of these natural scientific processes to develop techniques for separating the essence of molds and matching the residual liquid to a commonly used chemical substance called oxyacid. She also established isolation procedures for many disease materials that were sent to the lab.
The Penicillin Project team experimented with many molds from all over the country, growing them in a potato soup liquid. But, says Johnson, it was a mold on some cooked squash in her refrigerator at home that tested out to be the one that killed the germs.
Johnson was particularly interested in treatments for scarlet fever because of her experience with the baby who had died from the disease at the St. Louis hospital. Toward the end of the project, she conducted experiments with a tomato soup mold, testing it against specimens of saliva from an infant who had succumbed to scarlet fever. This particular penicillin mold turned out to be such an effective devourer of scarlet fever germs that Johnson nicknamed it “the terrible mice mold,” because under the microscope the mold looked like it was “running around the house tasting everything.”
After she discovered that penicillin was a viable treatment for scarlet fever, Johnson gave her results to one of the researchers with whom she worked in the lab, to take to the pharmaceutical company where he was employed. She left her final mark on the project by giving this advice: “Make the medicine up in peppermint-flavored syrup for babies and children, to be given around the clock until the fever breaks.”
Africa and Advocacy
But Mattiedna Johnson’s exceptional contributions to medicine and nursing didn’t end there. After completing her work on the Penicillin Project, Johnson embarked on a new chapter in her life. She received American Red Cross certification and began teaching disaster nursing and first aid. After the war, Johnson and her husband, a Methodist minister, spent two years in Africa, where she worked as a medical missionary in Liberia. She also taught chemistry and hygiene courses at the College of West Africa in Monrovia.
“My father’s hope for me when I was born was that I would become a medical missionary and go to Africa to serve,” she explains. “So this was a continuation of that promise my father made to God.”
Johnson and her husband eventually returned to the United States. Because of her husband’s many church assignments, they moved frequently. In 1959 they settled in Cleveland, where she tutored nurses for the Ohio Board of Nurse Education and Registration and worked as an American Red Cross volunteer. She also taught courses on babysitting and home nursing. But it wasn’t long before Johnson again became involved in making medical history.
“Some other nurses and I were at the church one day and we decided that Rev. Kelley [Johnson’s husband] was having too many funerals,” she says. “He was having two or three funerals a week, and we wanted to find out what was killing these people. We decided to do a 575-person blood pressure screening at Cory United Methodist Church. That was the first time that blood pressures had been taken [at a location] away from a doctor’s office. After that, blood pressure screening became widespread.”
In her later years, Johnson became an active participant in the 21st Congressional District Caucus and the Congressional Black Caucus Health Braintrust, chaired by Ohio Congressman Louis Stokes. In this capacity, Johnson began speaking out on behalf of African-American nurses. Realizing how difficult the socioeconomic situation was for black patients and health care workers, she held a meeting of black nurses at a 1970 nursing convention. That meeting led to the formation of the National Black Nurses Association in Cleveland in 1971. (The NBNA is now based in Silver Spring, Md.) Johnson later organized the Cleveland Council of Black Nurses in 1973.
In addition, Johnson’s continuing concern about the problem of high blood pressure in African-American communities led her to become actively involved in the International Society on Hypertension in Blacks (ISHIB).
“Mattiedna Johnson has been a member of the International Society on Hypertension in Blacks for the past decade,” comments C. Alicia Georges, RN, EdD, FAAN, secretary-treasurer of ISHIB and a past president of the National Black Nurses Association. “She was the recipient of our community service award for her work in blood pressure screening and education in the greater Cleveland area. Mattiedna has been a true community advocate and community educator, long before it became vogue. Her dedication to improving the health status of minority communities is exemplary.”
Mattiedna Johnson may be only one person, but her contributions to health care and the nursing field have affected the lives of many, thanks to a father’s promise to God and a nurse’s dedication to humanity.
Author’s Note: To learn more about Mattiedna Johnson and her life’s work, read her autobiography, Tots Goes to Gbarnga, available online from Barnes & Noble at www.BN.com. The book can also be purchased directly from Johnson; for more information, email her daughter, Bobby Kelley, at [email protected].
In Saskatchewan, Canada, the most rapidly growing segment of the population is the Aboriginal (Native) community, which is expected to increase to 400,000 by the year 2040. The Royal Commission on Aboriginal Peoples estimates that in Canada as a whole, approximately 10,000 more Aboriginal health care professionals will be needed in the next 10 years to respond to the health challenges experienced by Aboriginal people and to meet this population’s preventive, diagnostic, treatment and rehabilitative needs. There is an especially strong need for more Aboriginal nurses and nursing researchers. Currently, less than 1% of registered nurses in Canada are Aboriginal.1
The Nursing Education Program of Saskatchewan (NEPS)–a collaborative program of the University of Saskatchewan, the Saskatchewan Institute of Applied Science and Technology (SIAST) and, as of March 2003, the First Nations University of Canada–values research as a core competency for undergraduate nursing students. The program also recognizes the critical need to build Aboriginal nursing research capacity. For these reasons, NEPS has developed a capacity-building initiative that is supporting and enhancing research expertise among Aboriginal nursing students.
The students work with researchers, Aboriginal communities and NEPS faculty as part of an inclusive research environment. While the short-term outcomes are exciting, this initiative demonstrates even greater promise for building and sustaining research capacity for Aboriginal nurses over the long term.
Learning from the Literature
A review of the nursing literature indicates that a number of articles have been written about the process of building research capacity in organizations and institutions. According to a 1999 study by Jennifer Rowley published in the International Journal of Education Management, the first stage of research capacity building focuses on the development of research teams, personal growth, support and guidance for members of the team and a continuous learning environment. The second stage is the integration of these elements into the greater academic community. The study also states that “…research leaders have responsibility for establishing a sense of direction and for the facilitation of opportunities to support the individual learning of others.”2
Rowley lists the four key elements for successful research planning as ownership, objectives, outcomes and organization. She suggests that ownership requires a participative and collaborative approach to designing and monitoring the research activity: “Ownership can only be achieved if all researchers (from research students to professors) have involvement in the planning process, and, conversely, if all participants in the planning process are active researchers.”
The team needs to support individuals who are at varying stages of their educational development, Rowley notes. In addition, the team must have a sense of vision, a plan for the research activities that can be completed during an expected time frame, and must define the general purpose of the research, the subject focus and the anticipated networking. The outcomes should link to the objectives of the research and should be able to be disseminated through activities such as presentations, conferences, Web sites, student projects and publications. For success in building research capacity, an organization must have a strong infrastructure as well as strong, creative individuals who contribute to the overall research culture.2
Another, more recent (2003) study indicates that undergraduate nursing students are capable of performing qualitative data analysis with proper guidance and support. Furthermore, students at this educational level are able to apply the steps of a content analysis to data they collect and begin to conduct a thematic analysis.3 This study also found that there was “improved student performance in the subsequent research process course [and] in other courses requiring application of research skills.”
Other recent studies have found that teaching nursing students to conduct all parts of the research process, with guidance from professors, prepares them for the realities of health care practice.4, 5, 3
Building Capacity through Collaboration
Currently, close to 200 students of Aboriginal heritage are enrolled in the Nursing Education Program of Saskatchewan, representing approximately 14 % of the student population. NEPS is a four-year program leading to a Bachelor of Science in Nursing (BSN) degree awarded by the University of Saskatchewan. SIAST offers years one and two in Saskatoon and Regina; First Nations University of Canada, Northern Campus offers years one and two in Prince Albert; and the College of Nursing, University of Saskatchewan offers years three and four in all three cities.
[ads:education]
SIAST’s Native Access Program to Nursing (NAPN) is a nationally and internationally recognized recruitment, support and retention program and is a significant factor in the success of Aboriginal students in the NEPS. Student advisors (three at the Saskatoon site and one at the Regina site) provide academic and personal advisement, tutoring, mentoring and culturally appropriate counseling. The advisors are also available to assist students with childcare, housing and funding concerns.
Over the past three years, the NEPS faculty and NAPN advisors have been involved in a number of collaborative initiatives funded by Prairie Women’s Health Centre of Excellence and the Indigenous Peoples’ Health Research Centre (IPHRC). IPHRC funds research in the areas of Aboriginal women’s health and culturally respectful health care for Aboriginal people. It also funds Summer Undergraduate Research Awards for students.
Each of these initiatives has identified the development of research capacity in Aboriginal nursing students as a fundamental goal. Students who are interested in participating in research projects must have a successful academic background, be enrolled in a health science program and have an Aboriginal heritage. This goal is embedded in the conceptual framework for building research capacity in NEPS, which is based on the standards for research set forth by the Saskatchewan Registered Nurses’ Association (SRNA). The specific foundational competencies applicable for nursing students on research teams require that the students:
Demonstrate openness to new ideas, which may change, enhance, promote or support nursing practice;
Incorporate evidence-based knowledge from research in nursing and other disciplines into nursing practice;
Read and critique research articles and reports in nursing, health sciences and related disciplines; and
Participate in a variety of activities as part of a research team.6
The following examples illustrate how these four competencies are incorporated into the learning experience of the Aboriginal nursing students in the NEPS:
Openness to new ideas. Several of the Aboriginal students who are enrolled in the NEPS are involved in the research capacity building. They function as members of the research team and participate in processes that are responsive to the participating Aboriginal communities and the research context. The students are encouraged to challenge the status quo and explore new options and opportunities to approach the topic of interest.
As part of their self-assessments and feedback about specific research projects, some students have commented: “I came to understand how to address the political agendas of others”; “I had problems being able to suspend my own experiences as an Aboriginal woman as I looked at the research–so it challenged my beliefs” and “openness to new ideas is what kept this research group together and functioning.”
Incorporation of evidence-based knowledge.Health planners and providers working with Aboriginal communities are increasingly in need of the most current and reliable research information to guide their decision-making and planning processes. Through their research experiences, the Aboriginal nursing students participate in knowledge exchange, culturally respectful research processes and relationship building. One of the students working with NEPS faculty and members of a Native community stated: “The experience reinforced the principles of primary health care and how to apply them in my workplace and the community.”
Evaluation and critiquing of existing resources.For each research project, student members of the team are assigned a primary area (topic of interest). For example, an emerging challenge in the area of research ethics in Aboriginal communities sparked an interest for one student, and she subsequently worked on the identification, collation and critique of the extant literature. Other students have conducted literature searches related to culturally competent care, community development and decision-making, and Aboriginal research methods. The knowledge the nursing students gain from this process contributes to the development and further refinement of research questions and methodologies.
The students have learned that conducting literature searches and reviews is a valuable experience. Their feedback reflects this: “Because of this experience, I now look for opportunities to participate or initiate research on my practice unit”; “I hope I can be an example to others as they watch me give care that is respectful and equal across cultures” and “I feel I have been rewarded with the knowledge I have taken away from this experience.”
Inclusiveness in the research team.The students are mentored by faculty through all phases of the research, from grant writing to dissemination of research results. Several of the Aboriginal nursing student researchers have been successful in obtaining undergraduate grants from the IPHRC and from Health Canada’s First Nations and Inuit Health Branch (FNIHB) to facilitate their development in health care research. The students have told us that being members of the research team is “a great learning experience. . . [I am] learning how to prepare documents for an ethics committee” and “this collaborative effort definitely gave me more insight on working with others for a common goal.”
Showcasing Students’ Success
Through a coordinated approach and organizational support at all levels, the ongoing development of research capacity with the Aboriginal nursing students remains a priority in the NEPS. Summer studentships, research assistant opportunities and community linkages all contribute to the eagerness of the students, the ongoing commitment by faculty and the positive response from the local Aboriginal communities.
The nursing students’ successes as researchers have been showcased through publication, presentations, newsletters and posters. This past February, three undergraduate students and one graduate student participated in a student panel as part of Research Day at the College of Nursing, University of Saskatchewan. The feedback from participants at the Research Day indicated a very positive response to the student presentations.
The momentum and positive energy from these research initiatives are contributing to new projects and grants and are enhancing the learning of all members of the research team. Moreover, the research capacity building continues even after the students graduate. One recent graduate has already enrolled in a Masters of Nursing program. Another continues, as a registered nurse, to be involved in funded research related to community development within an urban Aboriginal community.
These Native nurse researchers are leaders in both the nursing community and in the Aboriginal communities. They are demonstrating the positive impacts of research on the health of their patients and the enhancement of culturally sensitive nursing practice. The Cree word Sihtoskatowin captures the value of working together on research projects, providing ongoing support and building research capacity with Aboriginal nursing students.
Acknowledgments:
The authors would like to thank the following Nursing Education Program of Saskatchewan (NEPS) students and graduates who provided statements that were used as quotes in this article: Alex Keewatin (student), Dwayne Nagy (graduate), Andrea Pouteau (student) and Nora Weber (graduate).
References
1. Royal Commission on Aboriginal Peoples (1996). Report of the Royal Commission on Aboriginal Peoples. Retrieved from http://www.ainc-inac.gc.ca/ .
2. Rowley, J. (1999). “Developing Research Capacity: The Second Step.” International Journal of Educational Management, Vol. 13, No. 4, pp. 208-212.
3. Reising, D.L. (2003). “Establishing Student Competency in Qualitative Research: Can
Undergraduate Nursing Students Perform Qualitative Data Analysis?” Journal of Nursing Education, Vol. 42, No. 5, p. 216.
4. Fazzone, P.A. (2001). “An Experiential Method for Teaching Research to Graduate Nursing Students.” Journal of Nursing Education, Vol. 40, No. 4, pp. 174-179.
5. Neafsey, P.J. and Shellman, J. (2002). “Senior Nursing Students’ Participation in a Community Research Project: Effect on Student Self-Efficacy and Knowledge Concerning Drug Interactions Arising from Self-Medication in Older Adults.” Journal of Nursing Education, Vol.41, No. 4, pp. 178-181.
6. Saskatchewan Registered Nurses’ Association (2000). Standards and Foundation Competencies for the Practice of Registered Nurses.
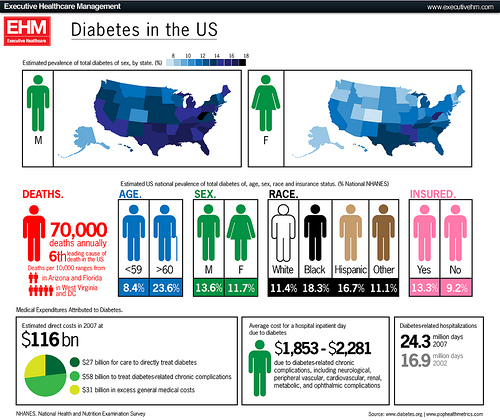
Several recent articles in Minority Nurse have examined how the emerging field of health care genetics and genomics has begun to revolutionize the way researchers and clinicians are working to eliminate racial and ethnic disparities in health outcomes. Being able to determine that a patient is at a genetic risk for developing conditions such as cancer and heart disease, and understanding the factors that can cause the patient’s genes to “express” (trigger) the disease, can result in more effective prevention and treatment strategies targeted to that person’s individual genetic makeup.
One of the most exciting new research projects to be launched in this area is an international collaboration that will focus on identifying the genetic factors that cause people to develop diabetes—a disease that has become a deadly epidemic among America’s minority populations. Digital Gene Technologies, Inc. (DGT), based in La Jolla, Calif., has teamed up with the French National Institute of Health and Medical Research (INSERM) for a groundbreaking study designed to identify gene markers and targets associated with the destructive T lymphocyte imbalance that leads to type 1 diabetes.
Spokespersons for the project describe it as “a bold, genomics-based approach to understanding the molecular mechanisms that lead to diabetes.” The French research team, led by Dr. Jean Imbert of the Institute Paoli-Calmettes in Marseille, will use TOGA®, a pioneering gene expression evaluation technology developed by DGT, to examine human blood samples from diabetic and non-diabetic populations and search for the genes responsible for the onset of the T-cell imbalance that initiates diabetes.
Dr. Imbert believes the study, when completed, will help focus attention on potential new targets for controlling and preventing diabetes. “We expect our results to reveal novel molecular signatures that may help us better diagnose at-risk subjects and to lead us towards new strategies for preventive intervention,” he says.
It all started with a conversation that took place in 1999 between the deans of two highly respected schools of nursing–one of them an Ivy League school, the other a historically black university. These two academic leaders shared a common, passionate goal: to introduce undergraduate nursing students from underrepresented minority populations to careers in advanced practice nursing and research. Today, their germ of an idea has blossomed into a highly successful collaboration that has been praised by the National Institute of Nursing Research (NINR) for its leadership role in addressing racial and ethnic health disparities and has been recognized by the National Institutes of Health (NIH) as a national model for nursing school health disparities partnership programs around the country.
Catherine Gilliss, RN, DNSc, FAAN, dean of Yale University School of Nursing in New Haven, Conn., and Dorothy Powell, RN, EdD, FAAN, associate dean of Howard University’s Division of Nursing in Washington, D.C., wanted to change the face of nursing research by encouraging talented minority students at the baccalaureate level to develop an interest in research, go on to graduate school and pursue doctoral degrees. The most effective way to accomplish this, the deans agreed, would be to immerse the students in research to help them understand the process. Empowered by that understanding, they reasoned, the students would gain confidence in themselves and in their ability to make a difference by becoming nurse scientists.
So it was that the Yale-Howard Scholars Program was born. Each year, the program brings a small, select group of Howard BSN students to the Yale campus to receive mentorship, training and research opportunities. The project’s original design involved an intensive six-week summer internship in which each Howard scholar was matched with a mentor from Yale–a nursing faculty member conducting funded research–with whom they would work closely.
In the summer of 2000, the first group of nurse scholars traveled to Yale for their internship. Five students from Howard University were chosen to participate. During that inaugural year, Yale covered all of the students’ expenses.
“That first summer,” Powell recalls, “we had to convince the students that this was a good thing to do. We chose good students who were considering graduate school and had an interest in learning about research.”
The students stayed at Yale in campus housing facilities, attended seminars, performed some community service and worked on projects with their mentors. Within the context of the larger research project, the Howard scholars had to identify a research question that they could look at more closely, then use the data from the parent project and transform it into a research problem involving minority health disparities. The students were responsible for studying the data, analyzing it and presenting their results.
“An Incredible Experience”
Nicole Laing, RN, BSN, was one of the first Howard University scholars to attend the internship program at Yale. Her research project focused on type 2 diabetes in minority women.
“I originally wanted a clinical experience but was offered the opportunity to learn about research at Yale, so I went. I thought it would be a good experience and would prepare me for graduate school,” she says. “It was an incredible experience. I enjoyed my mentor’s approach. I was introduced to the research project and encouraged to just dive in. I appreciated being able to run with it.”
Laing graduated from the BSN program at Howard in spring 2001 and is now a graduate student at Yale, studying to become a Child and Adolescent Psychiatric Nurse Practitioner. “I love it!” she reports. “I’m having a good time and learning a lot. For minority nurses especially, the impact we can make on health care is so great. It’s worth the time and effort required to complete a graduate school education.
“Attending the Yale-Howard internship program definitely fueled my desire to go to graduate school and to attend Yale,” Laing adds. “The internship experience developed me both as a nurse and as a professional. It helped me prove to myself that I could do it, that I could attend an Ivy League school. Sure, it was challenging. But like anything else, I just had to make the commitment and do it.”
Making an Impression
At the end of their six-week internship, the inaugural group of Yale-Howard scholars presented their research at a symposium held at Yale. They had created PowerPoint presentations in which they demonstrated the application of statistics and their understanding of the research vocabulary to explain their findings. They fielded questions from doctorally prepared nurses in the audience. Everyone was very impressed at how well the scholars were able to articulate their research, says Powell. “Clearly, there was a transformation in these students,” she declares.
“Presenting my project was a challenge,” Laing remembers, “and it was wonderful! I actually understood the process and felt confident about what the numbers meant.”
But the research experience for the minority students didn’t stop when the six weeks were over and they returned to their own campus. To continue the process, the scholars were assigned Howard University mentors to work with them throughout their senior year. These faculty members attended Yale for three days to study the research being done by the Yale mentors so they could help the students continue their research during an independent study.
At the end of their senior year, the scholars presented their research findings to their own student body at the Howard University Carnegie Endowed Visiting Professorship and Research Day, an annual event where 350 people converge on campus to hear minority nurse scientists share their research. Here, too, the Yale-Howard scholars were very well received. “There was such pride and appreciation from their fellow students,” reports Powell. “The scholars did so well and it made a positive impact on their peers.”
One such peer was Angela McKnight, RN, BSN. “When I heard the scholars give their presentation, I felt encouraged. The following summer, I applied for the internship at Yale,” says McKnight, who participated in the Yale-Howard Scholars Program in summer 2001.
A Shining Example
From this early success, a ripple effect began. Students from Howard signed up for the next internship in droves. The program began to attract national attention. The Yale-Howard scholars became highly desired by some of the best graduate schools in the country; 75% of the students have gone on to pursue advanced degrees. The scholars were invited to present their research at the Howard University College of Medicine’s annual Biomedical Research Symposium. “The appreciation of the medical community on campus reflects the respect for the research culture developed in the nursing school,” Powell notes.
Deans Gilliss and Powell decided to bring their partnership program to the attention of the National Institutes of Health, in hopes of obtaining grant funding that would help them continue and expand the project. The agency was so impressed with the program that it agreed to provide funding for five years. In 2001, the NIH identified the Yale-Howard Scholars Program as a model partnership program for developing a pool of minority nurse scientists who can contribute to the elimination of health disparities. Since then, the program has provided a prototype for seven similar nursing school Partnership Center initiatives throughout the United States. (See page TK.)
The two deans agree that the benefits to both universities are great. “We have truly benefited from the relationship with faculty at Howard University, such as [learning from them] how to access [minority] participants for research studies and breach barriers in hard to reach populations,” Gilliss says. Adds Powell, “Yale’s influence helped us cultivate a research culture and a capacity for scientific education. We are experiencing an increase in applications to our undergraduate and graduate schools, attracting more students and faculty interested in research. And we are experiencing an increase in funding for research projects as well.”
Yale, which does not have an undergraduate nursing program, has also gained much from the fresh perspectives and cultural diversity that the BSN students from Howard bring to the campus. “Our faculty are more aware of how their scientific work can and should impact health disparities,” Gilliss explains. “It is exciting to have these extraordinary students on campus. There has been an increase in our graduate school admissions as well as an increase in faculty applications. Nationally, we are being recognized as an institution that values diversity in our faculty and student populations and that welcomes diversity of thought, culture and country of origin.”
Gilliss’ excitement is shared by the Howard scholars who have participated in the initiative, including the most recent group of four students who attended the summer 2002 program. The scholars are immersed in graduate- and doctoral-level culture. The seminars and networking events they attend pull them into the world of research and enable them to experience what happens at the higher levels of learning.
“I learned so much at Yale. It was an awesome experience,” recalls McKnight, who graduated from Howard University in 2002 and will be attending graduate school in the fall at George Mason University in Virginia. She wants to teach and, ultimately, become a nurse scientist conducting research in minority communities. “I am more critical of research studies now,” she says. “You can’t take the numbers at face value. You have to look at the sample used in the study.
“The partnership with Yale is opening doors for us,” McKnight continues. “We need more partnerships like this! This was a new experience for me as a person of color and as a student. I am excited to get involved so I can make sure that research is representative of and real for the minority population.”
McKnight says the hands-on research experience she acquired at Yale helped her truly understand what being a nurse scientist is all about. “The internship at Yale has opened my eyes to the possibilities,” she comments. “It has given me a greater understanding of how research works and how projects are determined worthy for funding. Research makes sense; without research, how will we know how new medicines, for example, impact our [minority] community if the members of our community are not involved in the research studies? Research is so important to our future and it is a critical part of nursing. We’re the ones who are on the front lines with the patient. Patients trust us. Our population needs us.”