Community colleges are experiencing an increase in the number of men pursuing nursing as a career choice. The National League for Nursing’s Annual Survey of Schools of Nursing for the 2010-2011 academic year indicated that 15% of associate degree students were males. At 15%, men enrolled in basic RN programs remained at the historic high reached at the beginning of the current economic recession. Across all levels of nursing education, approximately one in seven nursing students was male in 2011. This represents a 2% increase in the male student population since 2010.1These statistics are encouraging and provide a possible solution to the worldwide nursing shortage.
From Fall 2001 until Fall 2012, the Borough of Manhattan Community College (BMCC) enrolled 504 male nurses in their associate degree program. This increase in the number of male students has provided impetus for further examination of the reasons why more men are pursuing nursing as a career in the 21st century, and what faculty can do to support and facilitate the integration, progression, and success of male students in nursing programs.
A structured survey consisting of ten key questions was sent to 68 male students currently enrolled in the associate degree nursing program at BMCC. The survey questions were framed from general to specific in order to draw conclusions. A total of 52% responded and provided answers to questions such as:
The motivating factors for deciding on a career in nursing;
Influencing factors, such as type of work in the military and their decision to enter the health care field;
Personal reasons for choosing nursing, such as: job stability, better pay, career flexibility, and opportunity for advancement;
Work placement preference after graduation;
Resources that would be most beneficial to their success in nursing programs.
It’s a Man’s Opinion
Results of the first half of the survey have shed light on male student nurses’ view of their place and future in the profession. Demographic data related to male students indicated that 54% of respondents were in an age group of 35 to 44. Seventy-five percent (75%) of male students entered nursing after another career; 33% of male students had an associate degree in a field other than nursing; and 25% had a bachelor’s degree from a field other than nursing. Seventy percent (70%) had no previous health care experience. And 87% had no military medic background.
The second half of the survey focused on male students’ view of their place in nursing. Categories ranged from strongly disagree to strongly agree. Findings indicated that 70% of respondents expressed a desire to help others; 66% of male students had no knowledge about the history of men in nursing; and 45% believed that male nurses choose to work in specialized areas. These findings confirm the literature’s viewpoint that most male nurses tend to gravitate toward specialty areas.
Results of the last area of the study addressed the importance of having adequate resources to facilitate progression and positive outcome for male students. Most respondents felt that career counseling/internships (80%), academic tutoring in nursing content (74%), faculty mentoring (65%), personal counseling (60%), and financial aid (60%) would be beneficial to students’ progression and success in the nursing program.
Career Counseling/Internships. Career counseling is abundant in most colleges and universities, primarily for retail industries. Counseling for nursing students, however, focuses on how students can best prepare for graduating, passing the NCLEX exams, and achieving licensure.
With a drastic change in today’s economy, health care institutions have felt compelled to focus on creative ways of meeting staffing needs and cutting costs for orientating new graduates once hired. Due to the economic recession, nursing jobs are more difficult to secure. In addition, most hospitals require at least one-year of bedside nursing experience before hiring a new graduate. How will a new graduate acquire the experience necessary to land a job? The American Association of Colleges of Nursing reported that 88% of graduates from baccalaureate programs had jobs within six month of graduation.2 However, associate degree program graduates are not as fortunate. In order to adequately prepare for the workforce, associate degree graduates are counseled on the need to continue their education and to participate in an internship program during their final year of school or an externship program after graduation.
Colleges often apply for and receive grants in collaboration with hospitals to provide externship programs that will facilitate training and mentorship for new graduates. Most programs are limited to 10-15 students, depending on the cost for six weeks of training and mentorship. In this program, students are often given additional training in EKG, venipunctures, and physical assessment skills. Students must successfully complete the training program, at which time they receive job placement either at the institution of training or a sister institution within the same conglomerate.
Most faculty in nursing programs serve as counselors to nursing students and have an ongoing relationship with health care institutions to provide internships, externships, or volunteer residency programs. In these programs, students acquire more hands-on experience, which tend to be limited during the school year. All students, regardless of gender, receive career counseling and the opportunity to apply for internships or externships during the summer months. Students are also counseled to continue their nursing education, whether from an ADN-to-BSN or a BSN-to-MSN program. Most colleges and universities offer a free NCLEX review course to prepare students for the licensure exam. This serves as a win-win situation for students since most public colleges, including the City University of New York, pay for the cost for the three-day review session.
Tutoring in Nursing Content. Tutoring, mentorship, meditation, and relaxation have been categorized as stress-reducing resources that can be offered to students.3Students who are relaxed and adequately prepare perform better on exams. At BMCC, tutoring is offered each semester for all nursing students. A schedule is usually posted outside the tutoring room so students can plan to receive extra help with course content. At times, students who lag behind are placed with the more outstanding students in study groups, which form a basis of support for struggling students.
Additionally, course faculty is available during office hours to clarify content and to discuss any issue students may have. Male students are informed of the availability of our male faculty mentor, if they so desire to meet with him instead. Tutoring is also available through the e-tutor website. Students follow specific guidelines for submitting electronic questions and are required to be specific as to what help they need. Communication via e-tutor requires students to convey information such as assignment, textbook, edition, page number, and any other relevant materials that will help facilitate the process. Students provide a valid email address for ongoing communication and feedback.
Mentoring Opportunities. Addressing the need for faculty mentoring of male students focuses on the benefit of having professional role models. Ideally, male faculty can fulfill this role. However, only about 5% of full-time teachers in nursing school today are men.4One strategy that could provide mentorship for male students is to pair male students with male graduates of the program. For example, the American Assembly for Men in Nursing (AAMN) has initiated a chapter within the greater New York area aimed at providing networking and collaboration among the 17 colleges within the City University system. In other colleges and universities, developing bonds with non-traditional older male student mentors via establishment of mentorship programs is another means to foster a supportive environment for male nursing students.
Personal Counseling. Schools of nursing should readily refer male students to counselors to discuss problems that may impinge upon their educational experience. It’s preferable to assign a male counselor who can relate to the student’s issues. Faculty should look for red flags that may indicate a student’s need for counseling referral or a need for help with problem-solving issues. Implementation of counseling should be done early in the semester when problems first surface to avoid a point-of-no-return situation. The lead faculty could meet individually with the student after the first exam if the student does not pass, and the student can be given a choice to discuss the issue at hand with the faculty or see a counselor. The student should also be asked if they would prefer a male or female counselor.
Financial Aid. Obtaining a nursing education is expensive. The average annual cost for tuition, room, and board for the 2010-2011 academic year ranged from $8,085 at public two-year colleges to $32,617 at private four-year universities.5This does not include the cost of books, lab fees, equipment, and supplies. Additional expenses may include uniform, transportation to and from school, testing, and malpractice insurance fees. Financial concerns are some of the main reasons students struggle in or leave school.Students often are able to qualify for work-study, which provides extra cash for personal expenses. It is also possible to apply for grants and scholarships to offset the cost of tuition. Overall, some means of financing a nursing education is always available whether through state or federal funding. From time to time, small nursing incentive scholarships become available as well, which serves as additive means for helping students through a financial crunch.
Where Do We Go From Here?
A review of the literature has pointed to other areas in which faculty can have significant input in changing the culture of indifference towards male students in nursing programs. One such area is in the planning of clinical rotation experiences. Male students often begin their clinical rotation eager to apply theoretical concepts to clinical learning experiences. Sometimes, however, their emotions may overshadow their ability to learn. One such example is the maternal-child clinical rotation. Research suggests that male students are uncomfortable and have feelings of not knowing what to expect in the post-partum area. A beneficial strategy by faculty that could mitigate the situation is first being cognizant of students’ feelings and identifying male students’ concerns before starting the clinical rotation in any setting.
Male students may also have difficulty with the concept of caring and expressing emotion. Use of vernacular, which is broad and encompassing, would challenge misconceptions of male nurses as non-caring providers. Encouraging the use of gender-neutral language during discussions of concepts around caring would be beneficial to male students.6 Faculty can recognize that male students are able to demonstrate caring in a different way, such as touching a patient’s shoulder and providing words of encouragement—and they could show the same act of caring as holding a patient’s hand, which is so often done by female nurses.
A 2005 study published in the National Student Nurses’ Association’s magazine, Imprint, indicated that men considered nursing a “calling” and that they enjoyed “making a difference.” BMCC’s recent survey reveals similar findings. Clearly, there is a need for a change in faculty perspective of malestudents in nursing programs. Addressing the needs of male students calls for implementation of strategies that promote diversity and integration within the profession. There also must be a challenge to the public’s perceptions of males in nursing that create barriers for male students. Nursing leaders and administrators need to implement recruitment strategies that emphasize gender and racial diversity in brochures, nursing magazines, billboards, as well as in the media.7 Just as historically traditional male professions—such as medicine and law—have been altered over time by the entry of women and minorities, integrating more men into nursing programs allows the profession to proactively address the problem of gender imbalance within nursing.
References
1. Kaufman, KA. Findings from the Annual Survey of Schools of Nursing Academic Year 2010-2011. National League for Nursing. June 2012. www.nln.org/researchgrants/slides/exec_summary_1011.pdf.
2. American Association of Colleges of Nursing. Employment of New Nurse Graduates and Employer Preferences for Baccalaureate-Prepared Nurses. Research Brief. October 2011. http://www.aacn.nche.edu/leading_initiatives_news/news/2011/employment11
3. Moscaritolo LM. (2009) Interventional Strategies to decrease nursing student anxiety in the
clinical learning environment. Journal of Nursing Education 48, 17-23.
4. National League for Nursing. (2011). Re health affairs and the nurse educator shortage.
Retrieved from http://www.nln.org/aboutnln/blast/blast_health_affairs_response.htm
5. U.S. Department of Education, National Center for Education Statistics. (2012). Digest of Education Statistics, 2011 (NCES 2012-001), Chapter 3. Retrieved from http://nces.ed.gov/fastfacts/display.asp?id=76.
6. Patterson J, Morin KH (2002) Perceptions of the maternal-child clinical rotation:
The male student nurse experience. Journal Nursing Education 41, 266-272.
7. Roth, JE, Roth, Coleman CL. (2008) Perceived and real barriers for men entering nursing:
Implications for gender diversity, Journal of Cultural Diversity 15, 148-152.
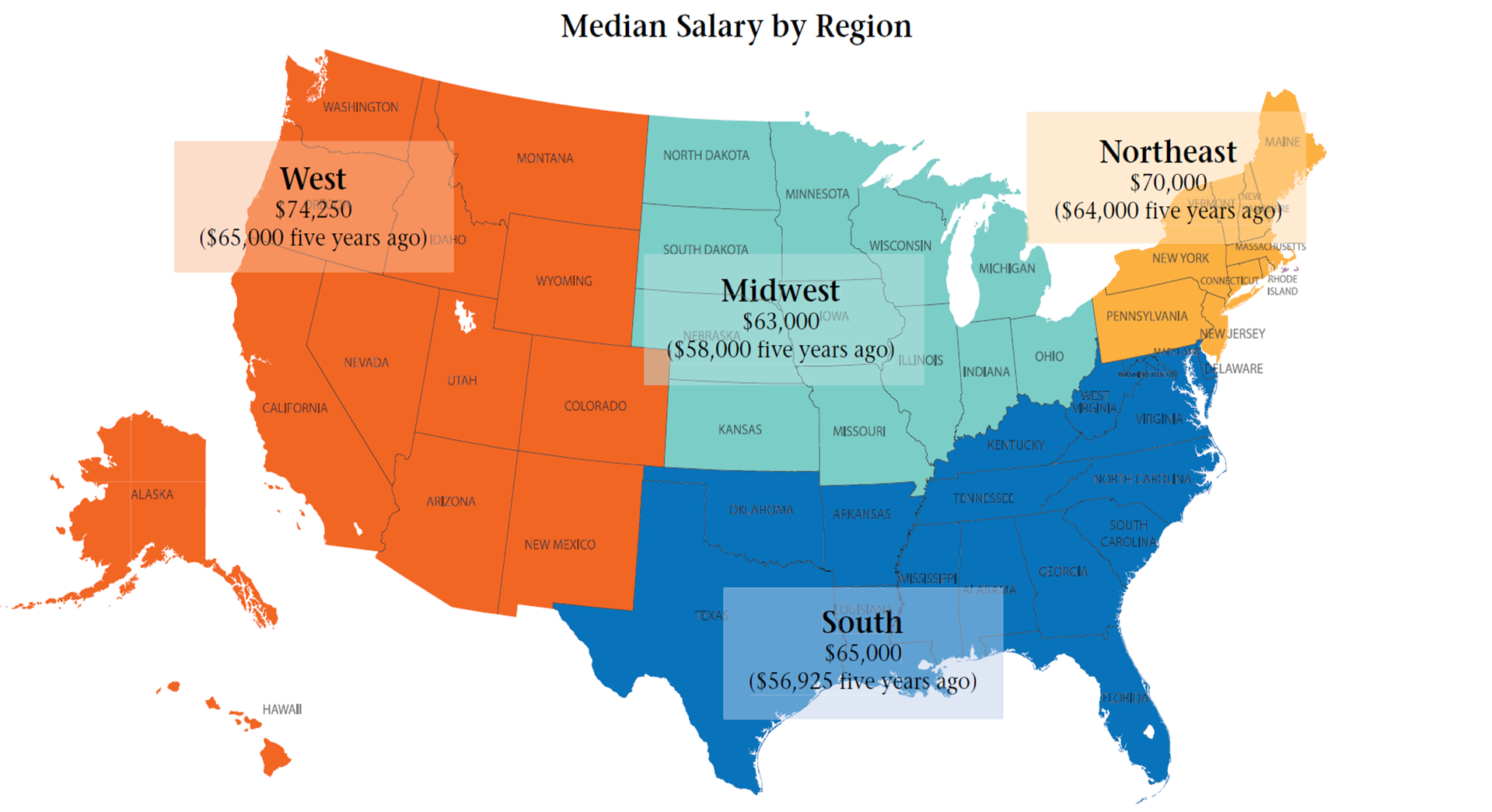
While there is a range in how much nurses earn, nurses reported making more money this year than they earned five years ago. Respondents to the first annual Minority Nurse salary survey reported an overall current median salary of $67,000 and said they had a median salary of $60,000 five years ago. Further, many, though not all, employers also offer benefits, most commonly health insurance and a retirement plan.
However, those values encompass all regions of the United States as well as a variety of specialties and other factors, including ethnicity and education.
For example, respondents living in the West reported the highest median salary, $74,250, while respondents living in the Midwest reported the lowest median salary at $63,000.
To gather all this data, Minority Nurse and Springer Publishing emailed a link to an online survey that asked respondents some 18 questions to characterize their educational backgrounds, main roles as nurses, and employer type, as well as to ascertain their current and past salaries. More than 3,000 nurses responded to this survey, representing every US state and the District of Columbia. The respondents also correspond to a broad swath of the profession, with nurses working in administrative roles or performing research as well as nurses tending to patients at their bedside in the NICU or in a psychiatric clinic.
Breaking the data down reveals some key differences in salary levels.
Median salary also varied by ethnic background. People of white/non-Hispanic backgrounds earned a median $71,119, followed by people of Asian descent making a median $64,000 and African Americans reporting a median $60,500. Hispanic or Latino/Latina nurses reported a median salary of $58,000 and Native American nurses earned a median salary of $60,000. Additionally, people who identified as multiracial reported earning $50,000, as the median.
Education also affected salaries as respondents with higher levels of education reported earning more in income. For instance, nurses with a bachelor’s level degree commanded a median salary of $65,000, while nurses with a master’s level degree said they earned a median salary of $70,000.
In addition, nurses with an advanced practice nursing specialization reported a median salary of $84,000. However, nurses with a medical-surgical specialization said they made a median salary of $55,000.
The good news, nearly all respondents reported earning more than they did just five years ago.
Highlights
23.2% of respondents have a PhD or other doctoral-level degree
43.7% work at a college or university
50.0% have been at their current job for five years or longer
63.2% received a raise within the last year
54.3% left prior job to pursue a better opportunity
45.2% do not expect a raise this year
49.1% are looking to leave their current job in coming years
For any student pursuing a nursing degree, the clinical rotations are where you really earn your pin.
“In clinical studies you put into practice what you learn in theory,” says José Blanco, MSN, MEd, RN, instructor in clinical nursing and director of the RN-to-BSN program at the University of Texas at El Paso School of Nursing. “The most important outcome is that you demonstrate that you know nursing—[which means] not only knowing the disease processes but also identifying signs, symptoms and treatments.”
There’s no denying that performing well in clinicals is a major challenge for just about any nursing student. But for minority students—including male students, as well as students of color—success in the clinical rotation often is linked to faculty members’ sensitivity to issues these students face that may differ from what non-minority students experience. It also can depend on adapting teaching strategies to diverse learning styles, advocating for students who encounter bias in the clinical setting, and creating effective interventions for students who run into obstacles or need to improve their performance.
The process begins with making sure students fully understand what they are expected to accomplish. While the overall objective of clinical studies is for the student to demonstrate competency in providing safe nursing care to patients, each clinical rotation has a different set of objectives, determined by the related course and the academic level of the student, says Emilia Frederick, MSN, RN, clinical instructor in the Department of Nursing at North Carolina Central University, a historically black university in Durham, N.C.
“The objectives students need to accomplish in a clinical rotation in their first semester as a nursing student are very different than the objectives students have to accomplish in their senior year,” she emphasizes.
Blanco notes that clinical students must learn to master a wide range of subject areas: pharmacology, I.V. therapy, transfer and discharge procedures, error and injury prevention, emergency response plans, safe use of equipment, infection control and patient rights. They also need to understand how to manage care and be an advocate for the patient, he says.
In addition, Frederick says, students must also become familiar with the particular standards and practices of the health care facility and unit where they are training—from the method of dispensing medication to the policies for interacting with patients’ family members.
Recognize Cultural Differences
One way instructors can help eliminate barriers to success in clinicals is to recognize different learning styles among students from diverse backgrounds.
“Many minority students, when we actually assess their learning styles, come across typically as sensory learners, as opposed to being analytical learners,” Frederick says.
Sensory learners need to have their senses engaged in the learning process, she explains. “If they don’t see it, hear it or touch it, it takes a long time for them to assimilate the information and be able to analyze it and apply it to the patient. If someone is an analytical learner, you can give them the information right out of the book and they are able to process it.”
While some studies suggest that sensory learners are especially prevalent among African Americans and other ethnic minority populations, Frederick argues that this learning style is not exclusive to those groups.
“We also have a generation of students who are from the computer age,” says Frederick, whose school has incorporated everything from simulation to YouTube videos and MP3 players to capture the attention of such students. “Sensory input is all that you get in the high-tech environment we’re living in today, so learning is really [becoming] more geared to sensory stimulation.”
Instructors also need to be aware that for some Hispanic students, cultural and language differences make the clinical rotation especially challenging, says Blanco, whose nursing school serves a large number of ESL (English as a second language) students. An even bigger obstacle for many of these students is time management. In addition to their nursing studies, many Hispanic students also have demanding family obligations, and they are also more likely to be working while going to school. At the University of Texas at El Paso School of Nursing, which has an 80% Hispanic student population, 75% of the students work, Blanco says.
Make Sure They’re Prepared
Perhaps no other success strategy is as important as making sure minority students are thoroughly prepared before they receive their clinical assignments. At North Carolina Central University, a pre-clinicals skills lab introduces students to the basic skill sets in which they will have to demonstrate competence. They also must pass a medication documentation exam before being allowed to mix and dispense medications to patients. Before each patient assignment, which comes with a 24-hour notice, the student must review the patient’s medical history and prepare a care management plan.
Global clinical training: As part of an elective course taught by clinical instructor José Blanco, MSN, MEd, RN (right), students from the University of Texas at El Paso School of Nursing traveled to a rural clinic in the mountains of Mexico, where they participated in reconstructive surgery.
“It’s important to clearly communicate the goals and expectations for students, and to be consistent with those expectations,” Frederick says. “It gets crazy when there’s inconsistency, or it’s constantly evolving. That creates a recipe for disaster.”
Ensuring that students get off to a good start can even involve something as simple as addressing transportation issues, according to Norma Martinez-Rogers, PhD, RN, FAAN, president of the National Association of Hispanic Nurses (NAHN) and associate professor/clinical instructor at the University of Texas Health Science Center at San Antonio (UTHSCSA) School of Nursing. “We have programs [at our school] that help students find ways to get to clinical sites,” she says. “We highly encourage carpooling.”
Advance preparation is especially critical for male nursing students entering the OB/GYN and pediatrics rotations. At the University of Portland (Ore.) School of Nursing, all students complete a skills lab before entering these rotations. But clinical instructor Kathleen Bell, MSN, RN, CSN, says, “The people who get the most out of it tend to be the male students. They like having an opportunity to role play. They like being able to practice on a doll how to diaper a baby, how to wrap the baby appropriately and how to hand the baby to the parents, because they may not have had real-life experience doing that. We also have patient simulation equipment available so that male students can practice performing a breast examination on the models. They can be shown how to use the peri-packs before they are in a situation where they have to do this with real people.”
The skills lab also devotes significant time to teaching labor support—“the old-fashioned things like rubbing backs, warm showers, foot massages [and generally] being able to help women cope with labor in ways that don’t involve the use of pharmacology,” Bell says.
To help allay male students’ fears that female patients might accuse them of sexually inappropriate touching, two other faculty members at the University of Portland School of Nursing have developed a video called “Intimate Touch for Males.” It explains the need for male nurses to approach sensitive OB examinations differently than female nurses—for example, “being aware of other females in the room and always doing a neutral touch before engaging in a very sensitive touch,” Bell says.
“We give [male students going into OB/GYN rotations] extra attention and time, because this is a particularly sensitive area and it may be difficult for them,” adds Bell, who asks for male students to be assigned to her courses because of her experience in helping them overcome gender-based barriers. “That being said, I find that the male students love OB, and they are always surprised. They expect that it’s going to be terrible, that they’re going to want to run screaming down the hall in the other direction—and they don’t.”
Another key practice at the University of Portland is to have instructors on the hospital site during students’ OB and pediatric rotations. “This is not our model in every other clinical setting,” Bell explains. “But because this is delicate information and just a big crisis time for families, we believe it’s very important to have the instructor there on site. It makes a big difference for students who come from a different culture or whose primary language is not English, and it’s certainly helpful for the male students.”
Stand Up for Their Rights
Unfortunately, there may be times when minority students encounter racial, cultural or gender bias in their clinical assignments, such as racist remarks from a patient or disparaging comments about male nurses from female RN staff on the unit. In the workshops Frederick conducts with nursing faculty from various schools, she tells them that part of their job is “to protect your students.”
“You have to know when you need to step in front of the firing line, so to speak, because there are certain things a student should not be exposed to as an entry-level student in nursing,” she maintains. “They haven’t learned the socialization completely yet. They are still getting their feet wet. If you don’t protect them, it can be quite a problem.”
Playing that protector role might mean talking with the unit staff about avoiding assigning problematic patients to students who are too inexperienced to handle them, Frederick says. She admits that it’s a delicate balancing act. “You have to be able to select the right patients to match the academic standing of the student but still give him or her a very realistic patient population to work with.”
Blanco stresses that nursing students must be trained to render competent care no matter what the patient’s attitude might be. “The student has to understand: You are not there to value-judge,” he says. “You are not there to stereotype. You are not there to share your values with the patient or give advice to the patient. You need to be an advocate of the patient.”
Martinez-Rogers concurs. “Unfortunately, students are not there to change the opinion of whoever they’re dealing with. They have to remain focused and stick with their goal. If [the problem] gets really bad, we advise students to go to [the faculty member] who is in charge of their course.” If a student does bring a legitimate grievance to the faculty, she adds, “we’ll support them.”
In Bell’s view, “skill and caring [transcend] cultures and genders.” Still, she concedes, even though male nurses have become a familiar sight in many hospital units, gender does make a difference for some patients, especially in the OB/GYN setting. Bell’s practice is to give OB patients the option to reject any nurse they don’t feel comfortable with, for whatever reason.
Intervene Early
What can instructors do to help minority students who are not doing well in their clinicals improve their performance? When and how should you intervene?
When faculty members see that a student is not performing well, says Frederick, “they need to intervene as quickly and as early as possible.” She tells her workshop groups to follow their gut feelings. When they sense that students are in trouble, it’s time to start observing them more closely and discussing their concerns.
Objectivity is paramount when evaluating student performance. “It cannot be based on personalities or on whether or not you like them,” Frederick says.
She recommends documenting the student’s deficiencies in writing, as well as each conversation with the student about how to resolve the issues.
“Students can be emotionally charged during these discussions, and they don’t always hear everything that you are telling them,” she explains. “You need to document [what was said] and have a witness.” She suggests bringing the student’s advisor in on the discussion.
Martinez-Rogers adds: “I think the faculty has a moral obligation the minute they suspect that a student is having a problem to work with that student one-to-one and refer the student to [sources for] help.”
That intervention might take the form of a tutoring or mentoring program, like the one at UTHSCSA School of Nursing that pairs undergraduates with graduate nursing students. Nursing schools typically offer a variety of resources to help students succeed. The challenge, according to Martinez-Rogers, “is trying to get [students] to learn that it’s OK to ask for help.”
In the Spring 2009 semester, Bell began teaching what she says is a unique course at the University of Portland, in which nursing students develop their own study plans in preparation for professional licensure. Students in the class review their performances on standardized tests, such as those administered by the Assessment Technology Institute.
“They get a report of the areas in which they are deficient,” Bell says. “It can be critical thinking. It can be leadership. It can be patient safety.” By observing patterns in their test results, the students are able to design a “care plan” for improving their own performance.
Having nursing instructors on site during clinical rotations is a major advantage, Bell adds, because they can assist in identifying ways to address a problem immediately. “It’s not one of those things [that should be] left to the nurse on the unit.”
To be effective, intervention must be both constructive and timely, Martinez-Rogers advises. “It doesn’t work to tell students they did [something] wrong if you don’t help them to find a solution,” she says. “[You shouldn’t be] telling students at mid term, ‘you are failing clinicals.’ It’s a little late.”
For any student, a nursing education requires a major investment of time, effort and, in many cases, money—and for minority nursing students, the sacrifices are sometimes even more significant. That’s why Martinez-Rogers believes that preparing minority students for success in clinicals—and other steps toward receiving their diplomas—is so important.
“These students work hard,” she says. “They spend a lot of money on their [tuition and] books. And none of them come to nursing school to fail.”
Various inequalities exist in structured social systems. Women, people of color, the uneducated, the poor, and those who face disabilities have often gone voiceless and powerless throughout history, and their struggles persist today. These groups of people are marginalized and face discrimination, prejudices, and sometimes oppression. Nursing, a profession predominantly populated by women, isn’t any different.
For the purpose of this article, discrimination will be defi ned “as a showing of partiality or prejudice in treatment, action, or policies directed against the welfare of minority groups.”1 Discrimination can happen anywhere a power imbalance exists between groups of people, such as in education, in social and political contexts, and even health care. In particular, “discrimination in the health sector is disturbing as it violates the basic principles articulated by care providers.”1 Generally, nurses experience discrimination based on their gender, race, lifestyle, and physical disability. In nursing, discrimination and oppression have lead to lower salaries, hostility from colleagues in the workplace, and unequal access to professional development training programs and career advancement opportunities.
Oppression, like discrimination, involves structural limitations—imbalances and inequities across groups causing constraints not only in the physical environment, but also in social relations, economic status, and political situation.2 When discrimination against a group of people is encouraged and consistently exercised by those in power, it causes unequal access to opportunities, thus leading to oppression. As power structures in society become more established, oppression becomes the norm. Thus, oppression occurs today not because society actively seeks to disempower some groups of people, “but rather because of the effects of societal norms, laws, and unchallenged assumptions.”3
In health care, a cultural imperialism exists such that the medical model—the physicians’ practices, views, values, and beliefs—is the dominant culture and the established norm. Nursing, as “the other group,” can be “viewed as both different and invisible and is devalued and objectifi ed by the dominant group.”4 Though times have changed, nurses continue to be an oppressed group as they have experienced repeated, widespread, and systematic injustice under a patriarchal system by physicians, administrators, and marginalized nurse managers.4,5 The forms of discrimination and oppression, as experienced by nurses within the profession and the health care sector, have been documented and analyzed below, specifi cally, gender discrimination, racial discrimination, lifestyle discrimination, and discrimination based on disability. In addition, this article will take a closer look at horizontal violence, an expression of oppressed group behavior evolving from years of oppression, fi nding implications for nurse leaders to empower nurses and nursing students.
Nursing in a male-dominated world
From a global perspective, nursing has been regarded as an oppressed profession, largely due to the fact that it is female dominated.6 Various patriarchal cultures around the world condone the unequal power relationships between men and women, favoring men.7 This gendered hierarchy of women in subordinate roles emphasizes male domination and marginalization of women in society.8 Historically, before the late 19th century, women who provided nursing care were either nuns or domestic servants. “Nursing was then an unskilled occupation, poorly paid, and disreputable,” a position held only by women of low social status.9
The unequal power balance between physicians and nurses has resulted in nurses keeping their voices silent while in the workplace. Nurses may not challenge physicians in the workplace, fearing confl ict, stress, or reprisal.8 This could become problematic, especially if nurses have concerns about harm to the patients. Churchman and Doherty conducted a qualitative research study in the United Kingdom on nurses’ views of challenging doctors’ practice in an acute hospital and found nurses still lack the confi dence to question doctors’ decisions. When dissent was warranted, nurses played the “doctor-nurse game” to appease the physicians; this “game” refers to the hidden manner in which nurses have infl uenced physicians’ decision making by providing information and making suggestions about patient care, without appearing to undermine a physician’s status.8
Gender discrimination
Gender discrimination refers to distinction, exclusion, or restriction made based on socially constructed gender roles and norms, those that prevent individuals from experiencing full human rights.10 In reviewing the literature, two types of gender discrimination in nursing were found. The fi rst type refers to the preferential treatment of men in nursing— specifi cally with regards to career advancements—and the second type refers to society’s view of male nurses, potentially leading to unequal educational opportunities for males.1,10
In a profession dominated by women, it seems puzzling that female nurses still face gender discrimination. In 2005, Statistics Canada reported there were 314,900 regulated nurses (which consists of registered nurses and registered practical nurses) in the country, and of these, 94.5% were women.11 This data is comparable to 2005 U.S. data, where roughly 5.9% of the nursing workforce is comprised of men. The proportion of male nurses in Australia and the United Kingdom is slightly higher at 7.2% and 10.1%, respectively.12 Indeed there is a signifi cantly lower number of men in nursing, yet they are disproportionately represented in management such that in the United Kingdom, approximately 45% of those in senior management positions and higher education courses are male nurses.1 Additionally, male nurses are reportedly higher paid and move directly into middle and upper remuneration brackets faster than their female counterparts.1,13
A survey conducted by Hader that collected information from over 1,500 nurse leaders from New Zealand, Canada, China, and Saudi Arabia revealed male nurses move into management positions at a younger age and faster than their female counterparts. The other type of gender discrimination in nursing involves the negative effeminate stereotypes society associates with male nurses. This may be because society as a whole views nursing as women’s work because it is a caring profession.14 The media’s portrayal of male nurses and physicians seems to be an accurate refl ection of society’s views of men in health care as well. In movies like Meet the Parents, in which the lead actor plays a male nurse, the character is perceived as less masculine. Conversely, male physicians are generally portrayed as confi dent and masculine in the media. There also tends to be a patriarchal stereotype in health care, where the physicians are viewed as leaders and nurses are handmaidens carrying out their orders.15 Male nurses may experience gender bias at work from their patients and colleagues or through social stereotypes that question the masculinity of men entering the nursing profession.16 Such stereotyping has lead to poor recruitment of males into nursing, as well as unequal access of male nurses in their training and education.
Gender discrimination towards male nurses can also lead to unequal access during nurse education and training. Kouta and Kaite reported male nurses were prohibited from training in obstetrics and gynecology due to gender bias, causing male and female nursing students to have different learning experiences.10 Similarly, Patterson and Morin found male nursing students were unable to participate in providing postpartum care to maternal patients.17 Other factors, such as the very low proportion of male faculty in nursing and limited opportunities to work with male nurses in clinical settings, were also reported to have contributed to the male nursing students’ perception of gender bias during their nurse training.10 Interestingly, a study conducted by Olawaiye, Shelton, and Withiam explored gender bias toward male resident training in vaginal deliveries at a community hospital, and the researchers found no difference between male and female residents’ experience.18
Racial discrimination
Society has used race to create distinctions between people based on visible or other shared characteristics such as skin color or religious affi liations.19 Racial discrimination involves hostility towards members of particular racial groups enacted within organizations and institutions. In health care and nursing, racial discrimination still exist. In 2002, The American Nurses Association published a study conducted by Bessent, who surveyed more than 5,000 nurses, including African Americans, Hispanics, Asians, American Indians, and Caucasians. The survey found minority nurses experience barriers to their progress in nursing, and “59% of African American respondents, 53% of Asian respondents, and 46% of Hispanic respondents” reported feeling they were denied a promotion because of their ethnicity.20 Results from the survey also identifi ed barriers to career advancements, which include educational, institutional, personal, and professional obstacles. This data is consistent with data from the United Kingdom. For example, in Kingma’s 1999 study, black nurses in the United Kingdom with matching qualifi cations and experience lagged at least fi ve years behind in career progression compared with their white counterparts.1 In addition, blacks and minority ethnic groups in the United Kingdom are underrepresented in nurse manager and senior leadership positions.21 Similarly in the United States, Hispanics and African Americans are underrepresented in nursing leadership positions when compared to the general population.13
Race also plays a role in nurses’ salaries in the United States. For example, among nurses earning more than $120,000 per year, more than 90% of these nurses are Caucasians; 4% are black, and only 2% are Hispanics or Asians.13
The Royal College of Nursing in the United Kingdom has acknowledged that institutional racism occurs in nursing.22,23 Nurses in the United Kingdom described their experiences with racism as being negatively stereotyped by colleagues and the public, having patients reject their care, and being excluded from various opportunities.23 In addition, research from Aston Business School and Lancaster University Management School in the United Kingdom both found National Health Service (NHS) organizations where bullied and discriminated against ethnic minority nursing staff reported poor staff engagement and patient experience. Nurses belonging to ethnic minority groups in the United Kingdom also reported unfair treatment in the workplace, such as being prevented from attending further training programs that their Caucasian colleagues would have otherwise been encouraged to partake in.24
Literature on racial discrimination in the United Kingdom and United States demonstrate that nurses belonging to ethnic minority groups do not have equal access to job opportunities, career advancements, and training programs when compared to their white counterparts.
Lifestyle discrimination
Society’s prevailing heterocentric view has led to oppression and discrimination towards the lesbian, gay, bisexual, transgender, and queer/questioning (LGBTQ) community. Consequently, LGBTQ nurses may be perceived as “invisible” members of the nursing workforce, ignored and underrepresented in professional organizations and pathologized in the nursing curriculum.25 This is supported by the fact that there is limited empirical literature on the experiences of LGBTQ nurses in the workplace.25,26
Heterosexual nurses’ negative attitudes towards LGBTQ nurses are referred to as homophobia, biphobia, and transphobia.25 LGTBQ nurses also experience discrimination from societal discourse and predominating heterocentric institutional values, beliefs, and practices. A study conducted in the United States by Randall as cited in Eliason et al., surveyed over 100 nurse educators and found 10% of the respondents thought lesbians should not be allowed to teach in schools of nursing. These negative attitudes towards LGBTQ nurses have led nurses to have concerns about disclosing their sexuality to coworkers.
A study conducted by Eliason et al. explored the experiences of 261 LGBTQ nurses in the workplace and found 22% of participants work in LGBTQ-unfriendly environments. Nurses in the study described experiences ranging from harassment and derogatory statements from colleagues about their sexual orientation to job losses or not having their contract renewed despite years of excellent performance reviews.25
Another study conducted by Giddings and Smith explored the experiences of lesbian women in the profession of nursing. Many of the participants experienced homophobic reactions not only from heterosexual colleagues but also from “closeted” lesbian colleagues. One participant argued that lesbian nursing students chose to not disclose their sexual orientation to their faculty and classmates for fear of discrimination or being labeled as deviant. None of the participants discussed experiencing discrimination for career advancement because of their sexual orientation.
Disability discrimination
Having a disability presents many challenges for nurses and nursing students. There have been reported situations in which HIV-positive nursing students or nurses were expelled from their programs or terminated from their employment.1 The U.S. Equal Employment Opportunity Commission and the Americans with Disability Act defi ne disability as a “physical or mental impairment that substantially limits one or more of the major life activities,” including having a record and being regarded as having such an impairment. As recorded, the two major types of disabilities that put nurses in a disadvantaged position are learning disabilities and physical disabilities.
Research has revealed that nurses with physical disabilities sometimes feel compelled to leave the profession for fear of not “pulling their weight” or putting patients at risk. In a study conducted by Neal- Boylan that explored the exper ience of nurses and phys i c i ans with a physical and sensory disability, it was found that the nurses’ employment agencies did very little to accommodate the nurses’ disabilities or to retain them. In addition, the nurses reported the need to hide their disability from their patients and colleagues. Interestingly, both the nurses and physicians reported their colleagues seemed to have less compassion for them with regards to their disabilities, despite having a professional understanding of how the disability could be limiting them.27 Disability also narrows and alters career choices and trajectories for nurses with disabilities.
Nursing students with a learning disability may not have equal access to training programs that accommodate their learning needs. Although it is illegal for nursing schools to deny admission to an applicant because of a learning disability, nurse educators and mentors do not always have adequate knowledge on how to fully support the learning needs of students with a learning disability.28 Once admitted to the program, it is the student’s responsibility to inform the school of any disability and request accommodations.29 Yet, many students with a learning disability do not disclose it to their faculty for fear of being rejected or discriminated against.30 Generally, efforts to meet the needs of students with disabilities include extra time to complete examinations, courses, or the program as a whole.29 Modifying courses to best meet the learning style of the student is not always done. Studies have suggested that nursing students with a disability experience stigmatized and prejudiced attitudes from staff as well.30
Oppressed group behaviors in nursing
According to Freire, there are five salient dimensions of oppressed group behaviors: “assimilation, marginalization, self-hatred and low-self esteem, submissive-aggressive syndrome, and horizontal violence.”31 Oppressed groups assimilate the values and norms of the dominant group, believing they will gain acceptance, recognition, and power if they become more like the oppressor.31 For example, nurse leaders tend to adopt the values and norms of the dominant group in an attempt to achieve those goals. Successful assimilators, such as nurse managers and administrators, become marginalized from both groups, as they still exhibit behaviors of the oppressed group and therefore are not able to become full members of the oppressor group. The oppressed group develops low self-esteem and self-hatred as they continue to internalize the values of the oppressor group. Submissive-aggression syndrome occurs when the oppressed group feels anger towards the oppressor group but is unable to express those thoughts and feelings freely for fear of reprimand. This occurs when nurses constantly complain about hospital policies or the physicians they work with, but rarely confront the oppressors. The nurses, feeling powerless but still attempting to exert some form of control, engage in destructive behaviors toward one another, such as bullying and sabotage. This phenomenon is called horizontal violence, an issue that plagues nursing today.
The submissive behaviors of nurses towards hospital administrators and physicians have evolved throughout history, leading to horizontal violence. These acts do not only involve overt behaviors such as physical violence, but include subtle behaviors such as gossiping, eye rolling, belittling or criticizing colleagues in front of others, and isolating colleagues during group activities.5 Horizontal violence is prevalent in nursing, and it negatively affects not only nursing recruitment and retention, but also patient outcomes.32
Implications for nursing
There are many factors that contribute to oppression in nursing. Widespread change is needed in nursing, in the health care system, and in society at large to curb the problem. Empowering each nurse is a crucial starting point. For nurses, change must start with working toward developing the critical consciousness of nurses and other health care professionals. This would involve allowing issues to be brought to the forefront, refl ecting on the basis of generalizations and biases that inform thoughts and actions, and openly examining them.19 In this manner, individuals develop critically refl ective skills and consciousness begins by becoming aware of the extent to which they hold power, knowledge, and privilege in relation to other groups.19 Nurse educators can help their students develop a critical awareness by embedding refl ective exercises in the nursing curriculum, allowing the learner to engage in praxis.
To help decrease nursing bias, “nursing faculty members need to become sensitive to subtle incidents of gender bias that may have a signifi cant impact on student learning and success.” Nursing faculty must also become aware of male nurses’ contributions to the profession while evaluating texts, courses, and the curriculum for feminine nursing stereotypes.33
To foster an understanding of the unique expertise and scopes of practice of different health professions—of how individual professions fi t within the trajectory of patient care—inter-professional education and collaboration must occur.34 This is important to foster trust, respect, openness, and a positive attitude to other health care professions. Faculty in health care and hospital administrators must work together to create an environment that is supportive of inter-professional collaboration and education.
Within the health care setting, health professionals, including physicians, nurses, allied health, managers, and hospital administrators, must come together and develop policies to address discrimination, and eliminate abuse and disrespectful behavior in the workplace.5 Workplace diversity councils must be established to help support minority groups. There is also a need to develop programs to help minority nurses learn how to overcome discrimination “in the workplace, develop leadership skills that can open doors to career mobility, and negotiate with their employers to achieve more equitable treatment.”20 Health care leaders, including nursing leadership, must become more aware of the various resources available in the workplace and community to support nurses who are experiencing marginalization.30 Training programs need to be established to allow staff to become more aware of wider systemic issues (such as gender bias, racism, LGBTQ issues, and disabilities) that contribute to discriminatory practices towards various nursing groups.
From a research perspective, there is a need to conduct research that describes the marginalization of certain nursing groups and its impact on nursing recruitment, staff retention, and patient outcomes. To highlight the unique contribution of nursing, it is important to conduct research on nursing-sensitive patient outcomes. Studies also need to be developed to further examine how nurses view and understand oppression and their beliefs on the most effective ways to address this issue.4
Lastly, nurses need to resist the oppressive status quo that is pervasive in workplace cultures.4 If individual nurses question and resist the status quo, then, as a group, their voices become stronger
References
M. Kingma, “Discrimination in nursing,” International Nursing Review, 46 (1999), 87–90.
P. Stevens and J. Hall, “Applying critical theories to nursing in communities,” Public Health Nursing, 9 (1992), 2–9.
R. Northway, “Disability and oppression: some implications for nurses and nursing,” Journal of Advanced Nursing, 26 (1997), 736–743.
D. Dong and B. Temple, “Oppression: a concept analysis and implications for nurses and nursing,” Nursing Forum, 46 (2001), 169–176.
J. Longo and R.O. Sherman, “Leveling horizontal violence,” Nursing Management, 38 (2007), 34–37; 50–51.
M.J. Birks, Y. Chapman, and K. Francis, “Women and nursing in Malaysia,” Journal of Transcultural Nursing, 20 (2009), 116–123.
World Health Organization, “Health Topics: Women’s Health,” (2010), www.who.int/topics/womens_health/en/.
J. Churchman and C. Doherty, “Nurses’ views on challenging doctors’ practice in an acute hospital,” Nursing Standard, 24 (2010), 42–47.
L. McDonald, Florence Nightingale at First Hand, York Road, London: 2010 Continuum UK.
C. Kouta and C.P. Kaite, “Gender discrimination and nursing: A literature review,” Journal of Professional Nursing, 27 (2010), 59–63.
Statistics Canada, “National survey of the work and health of nurses,”
J. Daly, S. Speedy, and D. Jackson, Contexts of Nursing (3rd ed.), 2010 Chatswood, AU: Elsevier.
R. Hader, “Nurse leaders: A closer look,” Nursing Management, 41 (2010), 25–29.
D.M. Wilson, “Meet the Men Who Dare to Care,” Johns Hopkins Nursing, 7 (2009)
K. Lunau, “The enduring stereotype of the male nurse,” Maclean’s, (2011).
BC Nurses’ Union, “Men in nursing,” (2011)
B.J. Patterson, K.H. Morin, and N. Colby, “The experience of being cared for by nursing students after giving birth.” Paper presented at NLN Education Summit, San Antonio, Texas: National League for Nursing, 2003.
A. Olawaiye, J.A. Shelton, and M. Withiam-Leitch, “Is there gender bias toward male residents in an obstetrics and gynecology training program?” Journal of Reproductive Medicine, 51 (2006), 479–483.
J.L. Johnson, J.L. Bottorff, B.A. Hilton, A.J. Browne, and S. Grewell, “Recognizing discrimination in nursing practice: fi ndings from a study of South Asian women and their health care providers in British Columbia,” The Canadian Nurse, 98 (2002), 1–6
H. Bessent, (2002). Minority nurses in the new century. Washington, D.C.: American Nurses Association.
A. Waters, “Statistics reveal that BME nurse managers are under-represented,” Nursing Standard, 26 (2011), 9; 20.
N. Lipley, “Facing inequality,” Nursing Standard, 13 (1999), 12–13.
P. Kendall-Raynor, “Action plan to support black staff as research shows racism persists,” Nursing Standard, 22 (2008), 6.
J. Myers, “Career progression is not without prejudice,” Nursing Standard, 26 (2011), 1.
M.J. Eliason, J. DeJoseph, S. Dibble, S. Deevey, and P. Chinn, “Lesbian, gay, bisexual, transgender and queer/questioning nurses’ experiences in the workplace,” Journal of Professional Nursing, 27 (2011), 237–244.
L.S. Giddings and M.C. Smith, “Stories of lesbian in/visibility in nursing,” Nursing Outlook, 49 (2001), 14–19.
L. Neal-Boylan, “An exploration and comparison of the work life experiences of registered nurses and physicians with permanent physical and/or sensory disabilities,” Rehabilitation Nursing, 37 (2012), 3–10.
S. Tee and M. Cowen, “Supporting students with disabilities— promoting understanding amongst mentors in practice,” Nurse Education in Practice, 12 (2012), 6–10.
L. Helms, J. Jorgensenn, and M.A. Anderson, “Disability law and nursing education: An update,” Journal of Professional Nursing, 22 (2006), 190–196.
D.J. Wright and V. Eathorne, “Supporting students with disabilities,” Nursing Standard, 18 (2003), 37–42.
L.K. Matheson and K. Bobay, “Validation of oppressed group behaviors in nursing,” Journal of Professional Nursing, 23 (2007), 226–234.
G. Corbin and C. Dumont, “Defeating horizontal violence in the emergency department,” American Nurse Today, 6 (2011), www.americannursetoday.com/article.aspx?id=8314&fid=8276.
A.S. Anthony, “Gender bias and discrimination in nursing education. Can we change it?” Nurse Educator, 29 (2004), 121–125.
“Times and rules have changed a lot since I was first in nursing school back in the ’60s,” recalls Eddie Hebert, R.N., B.S.N., director of nurses at Louisiana State University Health Sciences Center in Houma, La. “However, many of the prejudices which males faced back then are still with us today.”
“For example, I was not allowed to enter the delivery room because I was a male student, but had to stand at the door of the room to catch a glimpse of the delivery,” he explains. “I was also not allowed to have a female patient. This all had to do with gender.”
Hebert also remembers studying textbooks that made no mention of the male gender—except as the patient. “All educational materials were oriented to the female gender,” he notes. “Males were seen in nursing texts as the anatomy to be studied—the one in need of female assistance. Every picture seemed to identify the nurse as the ‘caring female individual,’ while the patient was always a ‘male in need of care.’”
However, that was almost 40 years ago, some may argue. Certainly the bias and prejudices toward men in nursing that existed at that time no longer exist. Right?
Wrong, according to Gene Tranbarger, Ed.D., R.N., CNAA, associate professor of nursing at East Carolina University in Greenville, N.C. “Open discrimination against men is fast disappearing from schools of nursing but remains imbedded in the school fabric,” he observes. “The faculty still relies on feminine pronouns when discussing nurses. Male nurses who wish to work in obstetrics/gynecology still face obstacles and often have to resort to legal remedies.”
What about male nurses who happen to be racial/ethnic minorities? Do they face similar issues as non-minority male nurses, or do they experience a whole other array of issues? Though there is no single united viewpoint or experience that speaks for all minority men in nursing, theirs is a voice that is growing in strength and numbers. It is a voice that loudly proclaims the importance of the nursing profession reflecting the diversity of its patient population—including gender.
Lingering Stereotypes
Approximately 5.4% of the 2.1 million R.N.s employed in nursing in the United States are men, according to the National Sample Survey of Registered Nurses conducted in March 1996 by the Health Resources and Services Administration. Of these working male R.N.s, the racial and ethnic breakdown is:
“The last survey showed a progressively aging work force and that we needed to do more to encourage young people from diverse backgrounds to go into nursing,” says Vincent C. Rogers, D.D.S., M.P.H., the HRSA’s associate administrator for health professions. “The 2000 survey results will help us develop policies and programs to strengthen the nurse work force in practice and education.”
The survey also found that roughly 13% of students enrolled in nursing schools are men. Dwight Elliott, a senior in nursing at East Carolina University, is one of two men in his class of approximately 80 students. “I am the only black male in my graduating class,” he notes. “It has been kind of tough being a black male in a predominantly white female profession. I’ve caught some looks like, ‘What is he doing in nursing? He doesn’t look like a nurse.’ I feel like I must work twice as hard as others because one, I’m black, and two, I am a male.”
Elliott is not the only one turning heads as a male nurse. Ifeanyi John Nwokocha, R.N., B.S.N., a staff nurse at La Rabida Children’s Hospital in Chicago, recalls receiving a few strange glances himself while at a previous nursing job. He explains, “When I used to work in med/surg, I got reactions like, ‘Oh—a male nurse?’ I even got questions like, ‘Are you an orderly?’ People do not expect to see a black male nurse.”
Elliott agrees, noting that nursing has traditionally been a white female profession. “I feel that as more men come into nursing, [men as nurses] will become more widely accepted. My family and friends ask, ‘You want to be a nurse? Why not a doctor?’ I guess they feel that traditionally males are doctors and females are nurses.”
Stereotypes of nurses as being female and white have persisted throughout the years but do seem to be lessening as the number of minorities (including men) in the nursing profession has gradually increased.
Francisco Navarro, R.N., a nurse at La Rabida Children’s Hospital, has seen the effects of such stereotypes firsthand. “Some of the kids [I work with] have a hard time dealing with the fact that I am a nurse because they say that only women can be nurses,” he explains. This bothers Navarro, who believes the notion that only women are nurses is an idea the children learned from schoolmates or family. He also notes that society often labels male nurses as being homosexual.
To some extent, male nurses have been viewed as being different or gay due to their close working relationship with women combined with the assumption that nurses are female, believes Hebert. “For many years, nurses were considered the ‘handmaids’ of the physician,” he observes. “Today, things are a little different. Physicians have come to realize that nurses are much smarter than given credit for years ago. Nurses are now moving into higher management roles and are more educated than in the past.”
Hebert also feels that society is slowly becoming more comfortable with men as nurses. “Although people may feel a little uncomfortable at first sight of a male nurse, they will quickly come to trust and respect him for his professionalism.” He also believes that unlike female nurses, male nurses have had to prove themselves before being accepted.
“Because of years of publicity and propaganda, [the image of nurses] is fixed in the mind of the general public as being white and female and trustworthy. Minorities in nursing do not have this image.”
It’s Not Always a Man’s World
So how has the stereotype of the white female nurse affected minority men in nursing? The responses range from “a lot” to “not at all.” For Nwokocha, the stereotype has hurt.
“Right now where I’m working, they treat me with respect,” he says. “But in my experience, when it comes time for promotions, I feel like the male minority nurse lags behind.
“For example, when I worked in psych at another hospital, I was bypassed . Even though I knew the unit very well, they bypassed me and gave the position to another person. I feel like it was because I’m black and I’m male. All the promotions there were given to females.”
Bernard Smith, R.N., M.S.N., clinical educator and recruiter at Benjamin Rush Hospital in Syracuse, N.Y., observes that it is sometimes more difficult for male nurses to work in certain specialties (e.g., women’s health) than others. He remembers, “There was at least one physician (in obstetrics) who did not want us around his patients. He did not want any male nurses around his patients.”
Navarro agrees that it is harder for a male nurse to work in women’s health than in other areas of nursing. “I could never work in a maternity unit,” he says. “There was one instance while I was in school when I was asked to interpret for a new mother who did not speak English. My instructor was showing the mother how to hold her breast and the newborn so that the baby would latch on to her breast. I could tell that the mother was uncomfortable—she would not feed her baby while I was present. Her feeling uncomfortable made me feel uncomfortable; I felt as if I did not belong in that environment.”
Both minority and non-minority men in nursing face similar issues, believes Hebert. As a board member of the American Assembly for Men in Nursing, an organization for nurses to discuss and influence the issues that affect men in nursing, Hebert hears of the discrimination and harassment experienced by some of AAMN’s members.
“The fact that male nurses are not given equal opportunity to move up in the ranks or are being denied equal employment opportunities is repeatedly heard during our annual conferences by our membership,” he states. “Many male nurses are denied [the opportunity to work in] certain areas in hospitals, such as labor and delivery units, or nursery units. In my 30 years as a nurse, I have seen many unfair practices in which male nurses and minorities were passed up for promotions due to gender. This practice continues today and is slowly surfacing in courts throughout the country.”
Neutralizing the Gender Issue
At the same time, some men in nursing have experienced no repercussions from the “nurses are women” stereotype and have actually received positive treatment because of their gender.
For example, Ramon Lavandero, R.N., M.A., M.S.N., director of the International Leadership Institute of Sigma Theta Tau International, headquartered in Indianapolis, had a very positive experience working in obstetrics. As one of the first men to go through an obstetrics class at Columbia University’s School of Nursing in New York, Lavandero found the faculty to be extremely supportive, contacting him even before the course began to see if he had any questions or concerns about being the first (and only) male in the class.
“Some people might consider that favoritism because it wasn’t done for the women,” Lavandero says. “On the other hand, it was an acknowledgment of a new circumstance, and they were planning ahead.”
In fact, Lavandero was offered three different positions within the women’s health service after graduation. He believes his experience working in obstetrics taught him an important lesson about the role of gender in nursing. As he explains, “I learned that in great part, I had the upper hand depending on how I treated and dealt with other people. If I was comfortable and didn’t see my gender as being a distraction, then there was no issue. If I was assigned a woman as a patient and if I was at all unsure as I interacted with that patient, then it would become a question.
“So I would go in and say to the patient, ‘My name is so-and-so, and I’m the nurse who will be working with you today.’ Ninety-nine percent of the time, there was never any question. There were a few times when, for example, a mother in postpartum requested a female nurse because she felt she would be more comfortable with a woman. But we had set a very comfortable tone. I can’t really say I have problems because of my gender any more than a woman nurse might occasionally have a problem with a male patient.”
Lavandero agrees that there are stereotypes of women in nursing but emphasizes that there are stereotypes attached to many other careers. “There are stereotypes that soldiers in combat duty are men,” he points out. “Well, you know where that can lead in terms of stereotypes. In the same way, there are stereotypes of men in nursing just like there are stereotypes of women in nursing—just like there are stereotypes of women who teach physical education and of men in engineering.”
Finding Strength in Numbers
Given these stereotypes, what can men in nursing do to find camaraderie?
Join organizations that support men in nursing, encourages Hebert. “There is voice in numbers, and you should seek your special interest organization and see if they will stand behind you and support your issues of concern.”
One such organization is the American Assembly of Men in Nursing, of which Tranbarger is president-elect. “We are a small group of male nurses and their supporters and represent a wide diversity of age, educational background, work experience, sexual orientation, ethnicity and almost any other characteristics one can think of,” he says. “I look forward to each meeting so I can interact with others who share my work, my experiences, my concerns and my hopes for the future.
“I must also add that I enjoy greatly our dedicated women members who share our beliefs that nursing is a profession, not a gender-based occupation,” adds Tranbarger. “AAMN is a healthy organization of men and women and is better because of all who join us.”
Each year, AAMN holds a conference, rotating the theme so that one year focuses on men’s health issues and the next focuses on issues of gender in nursing. “Diverse Nurses for a Diverse World” is the theme of this year’s conference, which will be held in Seattle from November 30 to December 2.
Another organization which offers support to nurses is Sigma Theta Tau International, an honor society of nursing with over 120,000 active members. As part of the International Leadership Institute, the Chiron Mentor-Fellow Program was started in January 2000 to provide the opportunity for individualized leadership development to members of Sigma Theta Tau. Although there were not any men involved in the program at the time of this article’s writing, Lavandero states, “We very much would like to have men involved. We really would like it to be a very diverse program.” He encourages potential mentors to identify a potential fellow and to apply to the program as a pair, believing it to be a valuable way for an experienced nurse and mentor to help another person to develop.
Other sources of support can be one’s fellow nurses—both men and women; it is important not to adopt an “us against them” mentality and alienate those of the opposite gender. Smith urges male nurses to develop friendships with their female colleagues.
“By far, [female nurses] are going to be your greatest source of support and strength,” says Smith. “They always have been for me—just by the sheer weight of their numbers, if for no other reason. But it’s more than that. I’ve learned so much from the women who are colleagues of mine.”
Reflecting the Face of Society
In order to encourage other men to enter the nursing profession, Nwokocha speaks with high school students on an informal basis.
“I meet the students through my nephew,” he explains. “He introduces me to his friends: ‘This is my uncle. He’s a nurse.’ And the students come to me and say, ‘Oh, you’re a nurse? How do you like it? What’s it like being a male nurse?’ Some of the students are excited—they want to become nurses, too. But they also want to hear what it’s like from someone who’s a man. So I talk to them, giving them advice and telling them what nursing entails.”
Tranbarger believes the best way to encourage minorities (including men) to consider nursing as a career is first to speak well of nursing as a profession. “No one wants to join a group that dislikes their work,” he says. “We also need to make schools of nursing more welcoming to non-females and non-whites. Language, symbols and policies all need to give each person a full and fair chance at success or failure.
“I do not know a man who wants an advantage in nursing,” he continues. “Every man I know just wants a fair chance. I think that is true for other minorities as well.”
Lavandero offers some additional insight on this issue. “Rather than simply saying, ‘We need more minority nurses,’ I would phrase it as, ‘We need more men and more people from varied ethnic and cultural backgrounds in nursing because that is the composition of our society today.’ In general, what nurses really bring to the table is an ability to help identify the health care needs of the patients and families in our communities. If we are not representative of our [patient population], then it becomes a lot more difficult to identify and meet those needs.”