Good nurses are professionals who strive to make a positive impact in their organizations. Some are able to make this impact by working in planning with hospital administrators.
The minority nurse who works in planning is in a pivotal role for making sure patients are safe, says Evelina Echols-Sutton, BSN, RN, nursing director of Women and Children’s Services at Methodist Charlton Medical Center in Dallas, Texas.
These professionals often have leadership titles, such as nurse manager or nurse director. Or they may be in specialty roles, such as nurse statistician and nursing informatics, she says. But one common theme is that they are called on to share ideas with their organization’s leadership.
“They are in those key meetings where decisions are made on the policies that we adopt, the equipment that we eventually bring in to our facility, and the streamlined workflows that will make sure our patients and family are safe,” says Glenda Totten, RN, MSN, CNS, director of nursing services at Kaiser Permanente Los Angeles Medical Center in California.
On an average workday, a nurse who works in planning may interact with the director of pharmacy, information technology, environmental services, human resources, risk management, and legal departments, says Echols-Sutton. “My typical day is probably about four hours of meetings, four hours of office work, and then four hours of follow-up on all these activities.”
“Meetings are also a constant variable in my day,” says Sylvia Williams, RN, MSN, director of education and inpatient nursing services at La Rabida Children’s Hospital in Chicago, Illinois. “They range from brainstorming meetings on quality initiatives to troubleshooting staffing concerns. On average, I would say I am in meetings a good five to six hours per day. They are important to keep morale high and ensure everyone works together harmoniously.”
Kanoe Allen, RN, MSN-CNS, PHN, ONC, is chief nursing officer at Hoag Orthopedic Institute in Irvine, California. She says that nurses who work in planning have to juggle meetings with idea generation. “One of the challenges is carving out time to sit quietly and think through the issues and to have time to develop solutions,” says Allen.
Unsurprisingly, nurse leaders are better compensated for their efforts. The median pay for a nurse manager is $77,988, while it’s only $55,447 for a registered nurse, according to Payscale.com.
Hospitals in turn get someone who engages in positive relationships within nursing, and with managers, supervisors, staff nurses, and executive leaders, says Totten. “It takes all that to make it work and have a world-class facility.”
Managing Inside and Out
In addition to working with leadership, minority nurses in hospital planning also have to help manage their organizations’ external pressures, says Totten. There are numerous outside factors to consider, such as working to meet the standards established by the Joint Commission. As an example, Totten regularly conferences with a stroke performance improvement committee to help her facility earn a comprehensive designation from the Joint Commission.
“It’s ensuring that for any [stroke] patient that goes to our emergency room, or any that are inpatients, we react immediately. We get the neurology resident in there and get the team in there within seconds,” she says.
Totten also works on a nursing quality improvement committee to assess nurse sensitive measures, such as interventions that help prevent falls in the hospital. Her teams are responsible for coming up with tools to communicate with nurses so that they are quickly informed about any relevant changes within the medical facility.
“We plan for our 1,200 or so nurses to make sure that everyone, including the per diem nurses, know what’s coming, what’s changing, how they can get more education, and the kinds of tools they need so that they’re up-to-date with the changes,” explains Totten.
Another planning team is responsible for providing constructive criticism to nurses on meeting patients. This involves communicating the best ways to exhibit caring behaviors, such as pulling up a chair and sitting eyeball to eyeball with those they serve, says Totten.
“It’s evidence-based and proven that you don’t want to stand over [patients]. You want to be as close to them as possible,” she notes. “We’re trying to standardize how we greet our patients when they come in on admission and also while they’re here.”
These issues are important because of the new value-based purchasing environment, says Shawana Burnette, OB-RNC, MSN, CLNC, a nurse manager in High Risk Post Partum and High Risk OB at Carolinas Medical Center in Charlotte, North Carolina.
A portion of reimbursements received from the Centers for Medicare and Medicaid Services will be based on the patient’s value perception of the care they receive, she explains. This means nurses in planning have to encourage their teams to not only help the patient heal, but to also have a good bedside manner.
Another area where nurses who work in planning are called on to help is to find ways to improve infection rates. The Centers for Disease Control and Prevention as well as the Institute for Healthcare Improvement review these rates, and of course, the goal is to have them as low as possible, says Totten. “You have to plan how you can show that you have a stellar place.”
Medical centers also compete with other health care centers in the community. “The consumer is more astute nowadays, and they are open to shop for the best medical facility, best health care facility, and the best insurance,” she notes.
This means nurses who work in planning often need to represent their medical centers to the community. “We have a foundation that does fundraising. In order to help them, I have to go out and speak,” says Echols-Sutton. “You want to talk to those that you serve, and find out what’s important to them.”
Improving Soft Skills, Leveraging Clinical Skills
First, health care is a highly regulated industry. Second, reimbursements are based upon the customers’ perceptions of “soft” skills, explains Allen. “Putting the two together is a change for this industry.”
Fortunately, nurses are usually well-prepared. “Nurses, by their calling, have a set of innate behaviors of putting people and solutions to the front,” says Allen. “It is a team spirit, not an individual-only spirit. That is key to the success of multidisciplinary patient care.”
People come to nursing with a big heart and a desire to help others, and it serves them well in collaborative environments where they have to work together to find the solutions, she adds.
Allen notes that being successful in nurse planning requires emotional intelligence, meaning the ability to understand and have a sense of another person’s views. To achieve success in planning means being a team player, using that emotional intelligence to understand the interplay between various personalities and departments, and working in a collaborative manner to solve regulatory and other issues, she says.
Minority nurses who work in planning can also help bridge multicultural gaps. Multicultural environments are a challenge to blend and the goal is to bring out the best attributes, says Allen.
“We serve patients from many backgrounds and having a diverse staff allows us to better anticipate and understand their cultural needs,” notes Williams.
Soft skills are necessary in higher levels of planning, but practical experience is also important, explains Totten. “One thing you can never take away from a nurse is her clinical skills. It’s handy when you’re working in a clinical setting. The more you move up in your career, [the more] those clinical skills are key.”
It all comes down to ensuring that staff members have the correct resources to care for patients, says Allen. Providing the right resources allows the staff to provide strong patient care. “Staff who do not have to worry about resources and administration support provide great customer service,” she adds.
The Career Path
Minority nurses who want to work with hospital administrators, or who want to be in administration themselves, have multiple options.
“The best thing about the profession of nursing is you can pretty much take any path. You can be in a clinical track and still move up to administration. There is also the education track, nurse practitioner track, and advanced practice nursing,” says Totten. “All these elements can secure you a good position in administration.”
Totten’s own background is as a clinical nurse specialist, but she emphasizes there are many ways to advance.
As a first step, Burnette suggests becoming a bachelor’s-prepared nurse. “They have the four-year preparation that includes handling more professional issues and critical thinking,” she explains. “The classes prepare you to be in a leadership role.”
But you should also have your sights set on earning a master’s degree. “Years of experience on the nursing unit are critical, but I would strongly recommend to anyone that is interested in this path to pursue an advanced degree in nursing,” says Williams.
“Nurses who work in planning need knowledge-based skills like budgeting and financials, experience you don’t necessarily receive on the floor,” she continues. The more educated you are regarding the area you’re going in, the more prepared you will be.
Mentoring
Another important means for having a successful career in hospital planning is to find a mentor who can show you the ropes in a real life environment, notes Williams.
“There are many ups and downs in nursing. There are plenty of wonderful days, and there are days in which nothing seems to go right. Being able to balance the good with the bad is essential to having a long career in nursing,” argues Williams. A good mentor can instill these lessons to their mentees and help them find their way, she adds.
Mentoring is intended to help nurses develop their skills and grow within the nursing profession. “The mentor accomplishes this by sharing their years of experiences—warts and all—to help them see nursing in its true light,” explains Williams.
Mentoring also helps a person explore who they are and how they can achieve more in their career, says Allen. In some cases, it opens doors for opportunity as well. “I have had a mentor who challenges my thoughts and plans, refocuses me when I am at a loss and then cheers me on,” she continues.
Having a mentor can also help nurses develop critical work skills, such as priority setting, stress management, people management, and good communication, says Echols-Sutton. She hasn’t had an “official” mentor, but she has had role models she patterned herself after. Other nurses who aren’t in employee-sponsored mentor programs can do the same, she notes.
“I didn’t have just one person. I tried to learn from everybody, including coworkers, bosses, and even people out in the community,” says Echols-Sutton. “They were available for me to pick their brains.”
Burnette advises nurses to find mentors who are not necessarily in their departments. If you talk to someone who works in another area of the hospital, they can give you a more global view of your organization. It’s important to surround yourself with people who have different perspectives but who are committed to achieving the same goal of providing patients with the best possible health care, she adds.
Whether a nurse joins a formal preceptor program or starts an informal mentoring friendship, anyone who wants to work in planning should reach out to a health care professional with more experience to help them along, argues Totten. “It’s not just enough to sit in your position.”
Working with Administration
Hospital administrators face many challenges from staffing to budgeting, and it is impossible to have a “go alone” mindset, says Williams. That’s why nurses who are in planning are a vital part of the team. Nurses who work with hospital administration report that their careers are fulfilling, and they have a large say in improving their hospitals.
“When you’re working in planning, you’re able to communicate with all the various staff as well as patients. It gives you a love for the ways you can improve the care that’s delivered to patients,” says Williams. “That’s where you can make the biggest impact.”
Despite advances in recent years relating to cancer prevention, detection, and treatment, many minority groups in the United States continue to bear a greater cancer burden than whites.
According to the National Cancer Institute’s Center to Reduce Cancer Health Disparities, while one in three Americans will develop some form of cancer, it continues to be the number one cause of death for many minorities in the United States. Nationwide, African Americans have a higher rate of death from cancer than Caucasians, and cancer has surpassed heart disease to become the leading cause of death among Hispanics and Asian Americans in the United States.
While the statistics are sobering, researchers say minority nurses can play an important role in working to reduce cancer disparities in their communities.
“Nurses are at the forefront of care and can have a major impact in eradicating cancer disparities by educating patients about the importance of cancer screenings, early detection, and access to care,” says Kimlin Ashing-Giwa, PhD, professor and director of the City of Hope’s Center of Community Alliance for Research and Education in Duarte, California. Ashing-Giwa’s work focuses on addressing the disparities in treatment and outcomes between patients with different access and cultural approaches to medicine.
How Breast Cancer Affects African American and Latina Women
“Although African American women are less likely than white women to be diagnosed with breast cancer, they are more likely to be diagnosed at a later stage and to die of their disease,” says Ashing-Giwa. “Despite the decline in overall breast cancer death rates in the past 20 years, black women continue to have higher death rates.”
A 2012 report from the Centers for Disease Control and Prevention (CDC) says that mammography may be used less frequently among black women than white women. It’s also more common for a longer amount of time to pass between mammograms for black women. Additionally, Ashing-Giwa notes that African American women commonly have subtypes of tumors that are harder to treat, especially an inflammatory form called triple negative breast cancer.
The CDC report also stresses the importance of educating women about the preventive benefits and coverage provided by the Affordable Care Act, including coverage of mammograms without co-pays in many health plans and, beginning in 2014, expanded access to health insurance coverage for 30 million previously uninsured Americans.
“Additionally, a woman’s best overall preventative health strategy is to reduce her known risk factors for breast cancer as much as possible by avoiding weight gain and obesity, engaging in regular physical activity, and minimizing alcohol intake,” says Ashing-Giwa, who encourages nurses to talk to patients about their risk of breast cancer and the importance of getting mammograms and doing breast self-exams.
If women can’t afford a mammogram, there are many free resources available that nurses can recommend to patients (see sidebar). In addition, black women are less likely to get prompt follow-up care when their mammogram shows that something is abnormal. Waiting longer for follow-up care can lead to cancerous tumors that are larger and harder to treat.
Follow-up care after mammograms is also a problem for Latinas. “While Latinas have lower incidences of breast cancer than white or African American women, breast cancer is the leading cause of cancer death for Latinas,” Ashing-Giwa says.
A March 2013 study conducted at the Institute for Health Promotion Research at the University of Texas Health Science Center at San Antonio and published in SpringerPlus found that it took Latinas 33 days longer to reach definitive diagnosis of breast cancer than non-Hispanic white women. Researchers found that Latinas with abnormal mammograms benefitted significantly from the help of trained professionals called “patient navigators,” who were trained in providing culturally sensitive support. Patient navigators were also helpful in providing transportation, language, and childcare solutions.
“We need to move toward more prevention, screening, treatment, and follow-up that speaks to people in a language they understand,” says Ashing-Giwa.
Despite Being Preventable, Disparities Still Exist With Cervical Cancer
Also of concern are the large differences in rates of new cases and deaths from cervical cancer among African American and Latina women. “Latina women have the highest rates of cervical cancer, followed by African American women,” says Ashing-Giwa. “This is troubling because most cases of cervical cancer are largely preventable and treatable with regular Pap tests and follow-up.”
Mortality rates are also higher for women over 50.
“Many women believe that since they are single and not sexually active, they don’t need a Pap test,” Ashing-Giwa says. While stressing the need for older women to get regular Pap tests, she notes it’s also important for nurses to encourage younger women to get the human papillomavirus (HPV) vaccine and to use condoms. HPV infection is the leading cause of most cervical cancers.
“Cervical cancer should have been eradicated 30 years ago with the invention of the Pap test,” argues Ashing-Giwa. “Most women who are diagnosed with cervical cancer today are those who have never been screened for it.”
Minorities Less Likely to Get Screened for Colon Cancer
A 2012 study conducted at the Center for Health Policy at the University of Nebraska Medical Center College of Public Health and published in the public health journal, Health Affairs, found that minorities are less likely to be screened for colon cancer. The data revealed that 42% of Caucasians were screened for colorectal cancer, compared with 36% of African Americans, 31% of Asian and Native Americans, and 28% of Hispanics.
“The death rate for colon cancer has increased among African Americans and Hispanic people despite it being one of the most preventable forms of cancer, and if caught early, one of the most curable,” says Durado Brooks, MD, MPH, director of prostate and colorectal cancers for the American Cancer Society.
“Although many people of color are aware of colon cancer, they don’t always see how it applies to them,” says Brooks. “If they don’t have a family history of the disease or have symptoms, such as blood in their stools, they often don’t see the need to be screened.”
Only 10% of colon cancer cases are tied to family history, and by the time warning signs are apparent, the cancer has often progressed to an advanced stage where it’s harder to treat. And while it is currently recommended that regular colon screenings begin at the age of 50, it’s recommended that screenings for minorities begin at 45 since many colorectal cancers have been caught in African Americans and Hispanics at younger ages.
“Many people are unaware of the benefits of colorectal screenings,” says Brooks. “There’s the perception that cancer is a death sentence, yet up to 90% of colon cancer cases are preventable with screening.”
Brooks praises Kaiser Permanente for being proactive about screening its health plan members for colorectal cancer. “Rather than waiting for people to ask to be tested, Kaiser Permanente sends out fecal immunochemical testing kits, a type of fecal occult blood test, in the mail to their members who are 50 and older,” Brooks says. “Not all health care providers are as proactive with their approach.”
And while colonoscopies are still considered the gold standard for detecting colorectal cancer, they also require rigorous preparation—a point that prevents many people from getting tested. In an effort to increase testing for colon cancer, Brooks notes that it’s important to let patients know they have choices and that there are other screening options available.
A study published in the April 9, 2012 issue of Archives of Internal Medicine confirmed this by noting that patients were less compliant with screening for colorectal cancer when colonoscopy was the only option offered. Yet when patients were given a choice between a colonoscopy and fecal occult blood testing, 69% completed one of the two exams.
Latino Men at High Risk of Prostate Cancer
According to the American Cancer Society, prostate cancer is the most commonly diagnosed form of cancer among Latino men, and they are also the most likely to be diagnosed with later-stages of the disease.
A new study conducted by researchers at the University of California—Los Angeles (UCLA) and published in the March 2013 issue of Qualitative Health Research concluded that a combination of financial, cultural, and communication barriers play a role in preventing Latino men from accessing the care and treatment they need.
“These obstacles require a new focus on not only adequate health care coverage, but also on the array of hurdles that limit patient access,” says Sally L. Maliski, PhD, RN, FAAN, associate dean for academic affairs at the UCLA School of Nursing and senior author of the study.
Maliski cites inability to afford medical insurance, difficulty understanding insurance policies, a lack of health literacy among the men, and their limited proficiency in English as barriers throughout the entire prostate cancer-care process.
“Our findings made it clear that we need a system where not only is care affordable, but where we use a multi-faceted approach to improve access, increase health literacy, and greatly improve care coordination,” says Maliski.
Focusing on Cancer Disparities in the Asian Community
“The cancer burden in the Asian American community is unique because cancer has been the leading cause of death among Asian Americans for the past 13 years,” saysMoon Chen, Jr., PhD, MPH, principal investigator for the National Center for Reducing Asian American Cancer Health Disparities headquartered at the University of California-Davis Cancer Center. Chen adds that hepatitis B induced-liver cancer is the greatest cancer health disparity for Asian Americans.
“All Asian American immigrants and their children should be screened for hepatitis B to lead to earlier detection,” Chen says. “And Asian Americans who do not have hepatitis B immunity should also get the hepatitis B vaccine, [which is] the best way to stop the spread of hepatitis B.”
Chen and his colleagues have received a federal grant to increase screening for hepatitis B. Since December of last year, screening events have been held in Northern California at Asian health clinics, local churches, temples, health fairs, and community organizations.
Many Asian Americans don’t get regular cancer screenings, which also adds to poor cancer outcomes. “Until they have symptoms, many Asian Americans aren’t really concerned about cancer and don’t think screening is necessary,” Chen says. “Vietnamese women have the highest rates of cervical cancer, which can be detected and treated early through Pap smears.”
Chen says cigarette smoking is also a big problem among Asian American immigrants and that they are the racial group least likely to be counseled on smoking cessation.
“Smoking is the leading cause of death worldwide and it’s a preventable risk factor,” Chen says. “It’s a complicated message and often language can be a barrier. There’s a great need for smoking cessation programs that are culturally tailored to Asian populations, both in language and intent.”
Stomach cancer is also prevalent in Asian Americans and Chen attributes this to chronic infection with Helicobacter pylori bacteria, which is common in developing countries. In Koreans, diet is also to blame, specifically foods that are preserved with nitrates and nitrites, such as kimchi.
Since prevention and early detection are key components of cancer control, Chen recommends that nurses who work with different Asian American populations either learn the specific language of their demographics, or have cancer education materials readily available in different languages such as Vietnamese, Korean, Mandarin, and Tagalog.
“Nurses who can accommodate differences in language fluency, dietary practices, and cultural beliefs can help to remove some of the barriers that exist in screening and treating minority patients,” Chen says. “Nurses who have this expertise are often the bridge between health care systems and minority communities.”
Your favorite movie or TV show may feature a spunky heroine who’s smart, capable, and great at her job, but chances are she’s not a nurse. Although TV shows and movies are known to take artistic liberties with many professions—such as homicide detectives, lawyers, and politicians—the importance of what nurses do has been consistently downplayed and marginalized in mainstream media.
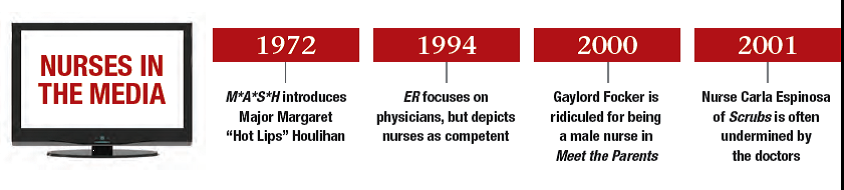
Historically, nurses have played a secondary role in health care-focused TV shows, perhaps showing up as the attractive “naughty nurse” or not featured at all. There were few prominent portrayals of nurses until the 1970s TV show M*A*S*H, whichintroduced Major Margaret “Hot Lips” Houlihan, played by Loretta Swit, to the popular culture. In addition to being the only main female character in the ensemble cast, Houlihan was an army nurse who served as romantic fodder for a few of the male characters over the course of the show.
But the majority of the media focus has traditionally been on physicians, with nurses serving as their handmaidens. “The media portrays nursing as a career for yesterday’s women living in the dustbin of history—women who just never got the memo that if you want to do anything of meaning in the field of health care, then become a physician,” says Sandy Summers, RN, MSN, MPH, who is the founder and executive director of the non-profit organization The Truth About Nursing, which seeks to increase public understanding of the central role nurses play in modern health care. “If the media knew that nurses actually perform intensely interesting and dramatic work and portrayed nurses doing it, the public would come to better understand—and respect—nursing.”
Recent Portrayals of Nursing
In the past decade, nurses have started to appear more frequently in entertainment, but the portrayals aren’t often reflective of reality. Summers says that unfortunately, the most popular shows that reach the largest audiences, such as Grey’s Anatomy, Private Practice, and House, tend to show physicians doing all the work—including tasks that are in reality performed by nurses—with nurse characters simply fetching things for the physicians. In real life, of course, the work nurses do is far more involved.
Manisha Ati, RN, BSN, is an operating room nurse at New York University Langone Medical Center in Manhattan. “During nursing interventions, nurses are making critical decisions without involving a doctor—decisions such as giving pain meds or escalating a patient’s situation if they’ve taken a turn for the worse,” says Ati. “I don’t think people realize what a complex and dynamic job nursing really is, just from watching media.”
The long-running TV hit ER (1994-2009) featured a large cast, but the emphasis was still on physicians. “Among the non-nurse shows, ER had good diversity of the nurse characters. There were Asians, African Americans, and men. Sadly, all were minor characters existing at the edges of the plot,” says Summers.
In recent years, more nurse-focused TV shows have cropped up, including Nurse Jackie, Mercy, and HawthoRNe, although Nurse Jackie is the only one that’s still on the air. “All three shows had good ethnic and gender diversity of nurse characters,” says Summers. HawthorRNe featured Jada Pinkett Smith in the title role of Christina Hawthrone, and Mercy featured Jaime Lee Kirchner as Sonia Jimenez, both African American nurses. Nurse Jackie, which Summers says does show some depictions of strong, astute nurses, includes South Asian and Middle Eastern nurse characters. The hospital-set comedy Scrubs (2001-2010) also featured a Latina nurse, Carla Espinosa, played by Judy Reyes.
Similar to entertainment, news reporters tend to highlight physicians instead of nurses when covering medical stories. One notable exception was during the October 2012 coverage of Hurricane Sandy at NYU’s Langone Medical Center, where Ati works. When the hospital basement flooded and back-up power generators failed, nurses evacuated 260 patients, including babies from the neonatal intensive care unit, and the national news outlets picked up the story, citing the heroics of nurses who worked through the night to carry patients to safety. “Nurses are generally portrayed as being in the background. That’s what was unique about the news coverage of Hurricane Sandy—the media actually recognized nurses for doing the work of moving patients. Even President Obama acknowledged the nurses for what they did—and that’s the kind of work nurses really do,” says Ati.
Are Minority Nurses Stereotyped?
As a field, nursing is extremely diverse. “Different cultures and backgrounds are embraced in the nursing profession, and I think that’s good; it makes you a better nurse,” says Ati. Diversity in the nursing field also helps nurses deal with the myriad backgrounds and cultural differences of the patients they serve.
Sources say that while nurses aren’t shown enough in the media, minority nurses are being portrayed fairly, when they do appear. “It’s not so much that minorities are being stereotyped—nurses as a whole are being stereotyped,” notes Summers. Ati agrees: “It’s not that minority nurses are portrayed differently—it’s that nurses in the media are the minority!”
Male nurses in entertainment tend to fall into two categories, says Summers: the “boy toy” that promotes female power when women boss them around, or the medical school drop-out, as evidenced with male nurse Gaylord Focker in the Meet the Parents movies—who won the professional approval of his father-in-law only after his fiancée revealed that he had scored in the 97th percentile on the MCAT—and staff nurse Ray Stein on HawthoRNe, who failed the MCAT the first time and dreamed of going to medical school.
Taking the Reins of Media Perceptions
The landmark Woodhull Study on Nursing and the Media analyzed articles published in 16 US newspapers, magazines, and health trade publications from September 1997. Researchers found that less than 1% of magazine articles and less than 4% of newspaper articles referenced nurses—and such references were made mostly in passing, not mentioning a nurse more than once. The study concluded that it was up to nurses to take a more assertive role in the media, such as speaking at public events and writing more letters to the editor to correct misrepresentations of the nursing field in the media.
Diana Mason, PhD, RN, FAAN, Rudin Professor of Nursing at Hunter College, City University of New York, heartily agrees. Dr. Mason is the co-director of the Center for Health, Media & Policy (CHMP) at Hunter, along with her colleague Barbara Glickstein, MPH, MS, RN, a health journalist. They also host a long-running radio show called Healthstyles on WBAI in New York. Through CHMP, Glickstein is the lead on media training, running workshops that prepare nurses to speak to the media—or start media on their own, such as through a blog, Twitter, or Facebook. “As nurses, it’s our responsibility to show the media what nurses do. We focus on what patients need and want, and that’s an important perspective,” says Mason.
Mason cites the CHMP blog, HealthCetera, as a good nursing media source to follow. In addition, Mason is proud of the ongoing work from nurses who have been through the media training workshop of CHMP, such as Chelsea Savage, RN, and Nancy Rudner, DrPH, RN. Rudner, a nurse practitioner, writes a regular health column for the Winter Park/Maitland Observer in Florida. Savage, a nurse who is interested in health care reform, is active on Twitter and Facebook.
Among minority nurses who have been through the CHMP media training, Mason cites Angie Millan, MSN, RNP, CNS, FAAN, who is the immediate past president of the National Association of Hispanic Nurses, and Patricia Lane, RN, BSN, an African American nurse in Virginia, as star students. Lane, whose passions include health policy and continuing education, wrote an op-ed piece entitled “More patients now assured of help” for the Richmond Times-Dispatch in June 2012 to comment on the passing of the Affordable Care Act.
“Since nurses are the most trusted health care providers, we can relay important health information to patients in a way they can really understand,” says Lane in a phone interview. Furthering her media outreach, Lane was selected by the American Heart Association to be part of the Spotlight Speaker Series on Racial and Ethnic Disparities in Hypertension: Beginning the Conversation 2012-2014. “It’s a volunteer engagement and community outreach program that will run in 18 US cities from January to June 2013,” Lane says. “We’ll assign mentors to coach participants to decrease their high blood pressure numbers and work with them to achieve a healthy lifestyle.”
How Nurses Can Gain More Exposure
When it comes to the lack of nurses portrayed in the media, Mason says that the problem goes both ways. Although the media should feature more nurses, there are also some barriers from the nursing community. “We have to do a better job of preparing nurses and nurse researchers to speak to journalists,” she says. “Nurses need to be prepared to describe what we do.”
In addition, nurses may be reluctant to talk to the media. “Nurses don’t respond to journalists. Nurses may be afraid that they don’t have the right expertise or aren’t comfortable speaking to the media. The media need to recognize and value that expertise, but they need nurses to speak to, as well,” says Mason.
Mason notes that nursing journals and organizations also need to become more media-friendly. She served for over ten years as editor-in-chief of the American Journal of Nursing (AJN), where Mason continues in an emeritus position. Under her leadership, AJN became the journal most frequently cited in the public media. It’s also important to frame nursing conferences to make them easy for journalists to cover, which hasn’t been done in the past, she says.
“What we can do is more outreach with public journalists,” says Mason. “The change will have to come from nurses and those who are educating nurses, not from the media.”
Summers points to the “Take Action” page on The Truth About Nursing website where nurses, the media, and members of the public can seek to improve the media’s understanding of nursing. She says it’s important for entertainment writers to start with an accurate idea of what nurses do before they begin creating TV shows and movies that feature them. “We encourage the media to consult nurses as experts on health care shows and news articles instead of assuming that physicians are masters of all health care,” Summers says. “So much relies upon the media to just stop buying into stereotypical assumptions and start asking nurses about nursing.”
What It Really Means to Be a Nurse
If media perceptions of nurses aren’t what they should be, there are different opinions on how to address the issue. “Although there aren’t many representations of nurses in the media, I just accept that that’s the way it is. I know what I do and the impact I have on my patients,” says Ati.
One nurse working to fill the media void is Kathy Douglas, RN, MHA, who is chief nursing officer for API Healthcare and the president of the non-profit organization On Nursing Excellence, which works to improve the efficiency, well-being, and recognition of the health care workforce. Douglas wants the public and policymakers to better understand who nurses are and what they really do. “The media is lacking true representations of nursing. The power of the role isn’t represented at all. You only hear about nurses when there’s a shortage or a strike,” she says. Douglas conceived and directed the documentary NURSES: If Florence Could See Us Now, which took about a year from its inception to its premiere in Los Angeles on October 11, 2012. The documentary seeks to paint a real picture of nurses today.
Douglas and her team spent about four months filming. They interviewed 120 nurses in nine different states, and of those, 73 nurses made it into the film. Douglas says there was no script she followed. “I would show up with a camera and interview nurses based on their specialty,” she says. “It was spontaneous, authentic, from-the-heart speaking.”
The NURSES documentary focuses on a wide variety within the field, including pediatric nurses, nurse educators, nurse practitioners, geriatric nurses, military nurses, critical care and trauma nurses, and nurse researchers, all sharing their stories of triumph and heartbreak. The goal of the documentary, says Douglas, is twofold: First, to educate the public, including the voting population and policymakers, to understand the role of nursing better. “People need to think of nurses not just when we need them, such as when we’re sick,” she says. Second, the documentary is for nurses themselves, to inspire and recognize them.
“I’m happy to share my story with others, to let people take from it what they will, which is hopefully a piece of hope or inspiration,” says Jonathan Van Nuys, RN, a nurse at Mission Neighborhood Health Center in San Francisco, who was featured in the film. Van Nuys was so moved by the support he got from a nurse named Laurie Mathers (also featured in the film) while he was a cancer patient undergoing chemotherapy that he was inspired to become a nurse himself. As an RN now, he works and volunteers to support people with HIV and is continuing his education to become a nurse practitioner.
During the filming, Douglas says her appreciation of nurses only increased. “I already had a deep respect for what nurses do, but it went to a whole other level.” Douglas was struck by how humble her interview subjects were: “I’m not sure they even know how amazing they are. It’s important for nurses to pause and recognize what they do.”
Douglas says that the reaction the filmmakers often got from nurses they interviewed was, “Who, me? I was just doing my job.”
“But that’s not the reality for those they touch,” she notes. Douglas adds that it shouldn’t take a crisis, such as Hurricane Sandy, to celebrate the work of nurses. “All the bad stuff in the news sells, but let’s talk about all the good nurses are doing.”
Nurses touch many lives, and this informs a unique perspective. “One of the deepest privileges of being a nurse provider is to sit as witness to people’s stories, their struggles, their vulnerability, their hopes and dreams,” says Van Nuys. Hopefully with more media created by nurses themselves and more media that seeks to have a true understanding of the profession, nurses will be able to do something they haven’t in the past— share their own stories with a larger audience.
See Our Champions of Nursing Diversity
Sign up now to get your free digital subscription to Minority Nurse