“Nurse practitioners are not, I repeat, not physicians. They lack education, IQ, and clinical experience. There is no depth of clinical understanding. They are useful but only as minions. Not politically correct, but true. Who would you want your family member seen by—a nurse or a physician?” —Doximity.com, 10/2017
One’s initial response may be to get angry after reviewing that. Yet, instead of remaining angry, perhaps the use of emotional intelligence and research could be of more benefit with analyses of the social media post.
A Little History Lesson
In 1965
, Henry Silver and Loretta Ford, a physician and a nurse, developed the first training program for NPs. The course of instruction focused on disease prevention, health promotion, and was in direct response to a national shortage of primary care physicians of that time. The deficit was especially concerning in rural, urban, and undeserved communities. This sounds eerily similar to current health care accessibility issues of today. Ford and Silver met much opposition with the development of the first formal program for NPs.
Surprisingly, the opposition was not only from physicians but also nurses. Some claim nurses believed that the title of “Nurse Practitioner” would be deceptive and somehow damage the nursing profession; meanwhile, it is believed that some physicians felt that NPs simply did not have the skills to take care of the public health needs without supervision (e.g., oversight). What is captivating, however, is how a nurse and a physician identified a need and were able to work in concert to try to address the concern.
The Un-Packaging
“Nurse practitioners are not, I repeat, not physicians.”
Merriam-Webster defines a physician as: “A person skilled in the art of healing.” Thus, this could be considered offensive to a physician who has gone to school for many years and has done an average of 10,000-15,000 hours of clinical rotation. In contrast, the NP goes to school for many years too but only averages 600-1,200 clinical hours. Humbly, if one is being honest, the sheer number of clinical hours that physicians do may suggest their training is better. Does that mean that they are superior? It should stand to reason that if one’s course of study includes more hours that their training is superior, but this does not mean that a NP is not essential in their own right. Therefore, it is understood that a NP is not a physician.
“They lack education, IQ, and clinical experience. There is no depth of clinical understanding. They are useful but only as minions. Not politically correct, but true.”
It has been documented that IQ tests do not test intelligence but can simply demonstrate that one is a good “test taker.” Hence, one should understand that having a high IQ does not constitute knowledge, nor is the IQ the only predictor for one’s success. The language used in the op-ed may be viewed as crude to some and offensive to others; however, if one could look past the words and get to the root of what was being said it might be helpful. Checking egos at the door and realizing that medicine is not a power structure—it should simply be patient-centered. As such, there may be some value to the thought that NPs need oversight to practice.
What’s wrong with collaboration, anyway? This should be viewed as a valuable tool that assists with the care and safety of patients who may not otherwise have access to adequate health care. This should not degrade the NP’s worth but prove valuable for the public.
For those arguing about NPs and their worthiness—are they willing to work in rural, urban, and undeserved areas? Who does this argument really hurt? To meet the current health care demands, there would need to be a tremendous supply of willing physicians. Where are they? Additionally, some studies imply women and children suffer the most in medically underserved areas, Who will serve them? Is that physician you?
“Who would you want your family member seen by—a nurse or a physician?”
Qualifications and experiences are probably the central reasons for patients preferring a provider no matter what their title. But physicians may be more often preferred for their skills, whereas NPs may be favored for their social skill and ability.
Maybe fear, lack of confidence, and overwhelming need as a NP to validate worth could make them seem unworthy. But this should not be confused with lack of skills or professionalism of the NP. Oversight should not indicate a servant-to-leader relationship but rather a teamwork concept to support and respect one another. One cannot reasonably argue with the number of hours of study a physician puts in—it is commendable. Having said that, this does not belittle the course of study for the NP, either.
Physicians and NPs are all valuable, and working together can be nothing but good for all around. So, in the words of Rodney King, “Can’t we all get along?” Let’s work together in concert to direct a beautiful symphony called safe patient health care.
Nurses are integral in the care of patients and their health. Exploring a plant-based diet may be beneficial to patients so they can take back their health. It is time for health care disciplines to be aware of a plant-based diet and to dispel any myths that exist. In fact, a plant-based diet is not a diet—it can be viewed as a way of life. A plant-based diet are foods consumed that is devoid of animal ingredients, such as dairy and meats. A plant-based diet relies on foods that are grown from the ground such as fruits, vegetables, whole grains and nuts, and seeds.
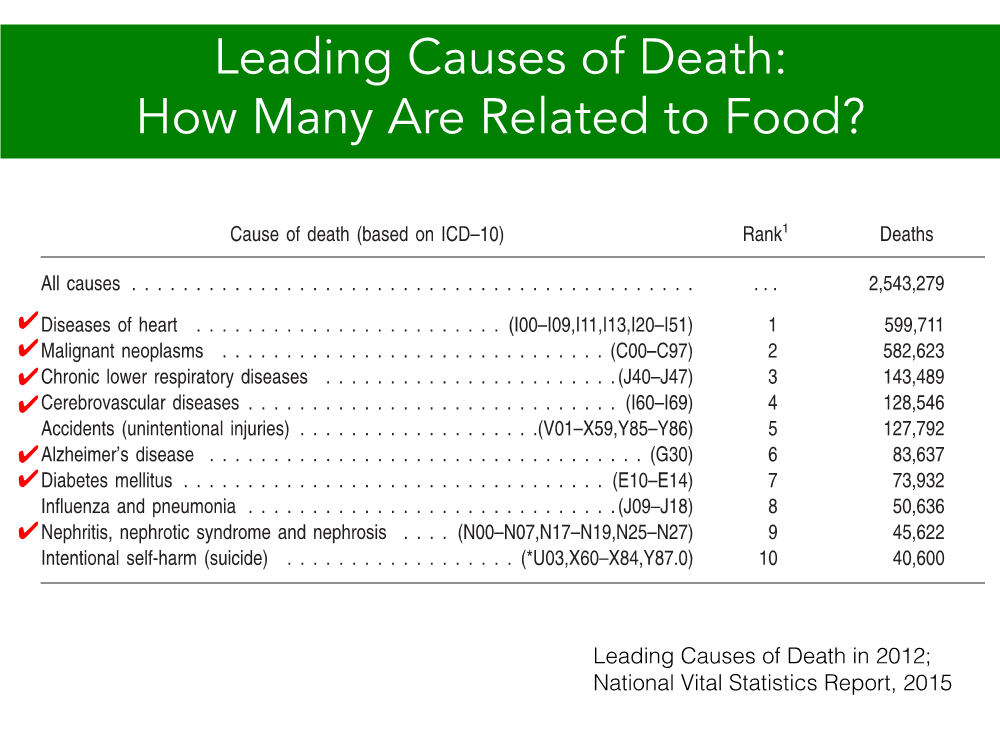
People are living longer, but we are also living with more chronic diseases, with heart disease being at the top of the list. Heart disease, diabetes, and hypercholesterolemia are contributors to sickness where medicine is the answer. Health care providers tell patients to lose weight by restricting food intake. While patients may see results initially, they usually do not adhere to this long term as it is not sustainable for them for a variety of reasons. In addition to that, the medications with their side effects usually do not highlight many benefits. One-third of animal products in the American diet are very concentrated in calories and are deficient in antioxidants and vitamins. Needless to say, the vast majority of chronic illness is highly correlated to what we eat. There is a different biological effect of meat versus plant-based protein such as beans. The body can store these amino acids and complete them without overshooting the hormone, Insulin Growth Factor 1 (IGF 1). On the contrary, processed foods and meats produce a lot of IGF1 where insulin ends up storing a lot of fat. It is also attributable to cancer and inflammation.
People have long touted the benefits of a
plant-based diet. Brooklyn Borough President Eric Adams reversed his diabetes Type 2 due to a plant-based diet. He was already suffering from nerve damage as a result of his disease with a hemoglobin A1C of 17 (anything over 6.5% is considered diabetic), so his was very high and the doctor was surprised that he was not in a coma. Adams was placed on medications, but he also sought the help of Caldwell B. Esselstyn, Jr., the same doctor who treated Bill Clinton and author of the book, Prevent and Reverse Heart Disease. He was informed by doctors that he would be on insulin for the rest of his life. He was placed on medicine for his acid reflux, medicine for his high cholesterol, and medicine for his burning and tingling of his hands and feet. His family is diabetic and was told that it runs in his family.
This past August, there was a launch of a plant-based lifestyle program at Bellevue Hospital in New York City. Doctors, nurses, dieticians, and life coaches will help at least 100 patients across all five boroughs adopt healthy eating patterns focused on legumes, whole grains, fruits, vegetables, nuts, and seeds while reducing animal products, fried foods, refined grains, and added sugars. Michelle McMacken, director of NYC Health + Hospitals/Bellevue Adult Weight Management Program, is director of the program.
At Montefiore Hospital, Dr. Robert Ostfeld spearheaded the Cardiac Wellness Program where plant-based nutrition is the prescription for management of cardiac disease. The population most affected by these diseases are non-white populations. Dr. Kim Williams, past President of the American College of Cardiology, advocates for a plant-based diet for heart disease prevention. Affronted with a high cholesterol, he decided to take measures into his own hands, and adopt a plant-based diet.
While medical doctors are beginning to advocate this lifestyle, nurses should also set an example of this lifestyle approach. Nurses are part of the health care discipline and minority nurses, especially, need to set an example. We want patients to take control of their lives. We can teach patients eating a plant-based diet instead of a standard American diet, as a form of primary prevention. Like any diet, it may take time to adjust, but this is not just a diet, it is a lifestyle. Patients would need to make an informed decision as to whether they would want to incorporate it into their lifestyle or not. There is enough supportive evidence out there that a patient can access such as documentaries, “Fork Over Knives” and “Fat, Sick, and Nearly Dead.” There are a variety of resources, including the 21-Day Vegan Kickstart program, to include in dietary prescriptions to help patients treat and prevent obesity, type 2 diabetes, and heart disease. This will require support from the patient’s primary provider, and, whether the provider is an advocate of this lifestyle or not, it should be considered. Benefits such as less medication, weight loss, and improvements in mood as well as cholesterol have been shown. Dispel the myths about a plant-based diet and protein.
This is a plea as something to consider to take better care of ourselves and take control of our lives. There have been many initiatives and programs to lose weight. Drastic measures have also occurred due to the outcomes of being overweight, such as drastic surgery and restrictions from carbohydrates. Patients are sometimes misinformed and have to get rid of the idea that medications will solve the problem—it only delays the problem. There is a possibility of reversing diabetes and cardiac disease. This is a decision that the person has to make: continue with their lifestyle with animal protein and processed carbohydrates or see a reduction in their overall weight and health by incorporating a plant-based diet.
A plant-based diet may be considered “extreme” by some people in altering their lifestyle. But given the choice between a plant-based diet or open=heart surgery, it can be posed to the patient which one they consider as extreme. Again, it is a personal choice, an evaluation of familial and cultural values would be assessed to fit the needs of the patient. Surgery can be viewed as a band-aid in that it will manage the symptoms temporarily unless the patient alters their lifestyle. Of course, it helps if the patient has a supportive network to embrace the lifestyle. It can start off as small, simple steps, as little as incorporating a plant-based meal in their day and slowly add these meals to their lifestyle. There are vegan starter kits to kick a healthier you.
Employment projections are estimating that Registered Nurse (RN) needs will continue to grow rapidly—at the same time a shortage in nurses is expected. Due to this shortage, it is critical for health care organizations to implement a firm training program, have direct leadership relationships, and target minority populations. Doing this will assist in filling RN openings and help create an organization that truly invests and cares for their nurses, which will positively impact retention.
Nursing school enrollment is not advancing fast enough to meet the RN demand, and with nurse baby boomers aging there will be fewer nurses available as the health care sector continues to grow. For example, in the Orlando, Florida region specifically, there are over 1,600 current RN job openings available, with 191 direct employers competing to fill those open positions. Simply put, there are not enough nurses to fill all those critical needs in the market. This shortage is impacting the current nurses’ job satisfaction, increasing their stress, and even driving some nurses to leave the profession.
Without nurses we cannot run our health care organizations, which is why having a process in place to train and support them is essential. To invest, you must have
a proper training program to support the nurse and ensure they are demonstrating safe quality care to patients. Certain organizations, such as AdventHealth, implement this in their Graduate Nurse Residency Program in the Orlando region. The first two weeks of the program are focused strictly on modules, simulations, and computer training. During that time the new nurse goes through a three-day simulation lab to provide hands-on learning before they even enter the department. The following months are focused on individual preceptor training. The nurse is partnered with an experienced nurse for a certain amount of duration (8-16 weeks depending on the acuity of the unit) to train the new nurse and will be with them every single shift side by side so they have the resources and training to be successful. After the focused preceptor training, the new nurse continues to be provided educational courses and simulations as needed. This shows the nurse that the company is investing in their future.
Proper training programs and support for nurse staff is essential for the nurse to feel like they have more opportunity, and desire to stay and grow as part of the organization. With the shortage of nurses, you need to ensure the nurses that you do have feel supported and uplifted to reach their full potential. Providing this training will provide a higher percentage of nurses to feel valued enough to want to stay in that organization and to have the desire to give back full circle to the organization that invested in their learning and education.
Leadership involvement is also a direct way for organizations to increase retention. If a nurse is feeling overworked, they need to at least feel appreciated for all they do. Open communication is critical for retention—and to really understand where your employees are coming from. Nurse leaders need to uphold regular one-on-one meetings and gain a professional relationship with their employees to understand their struggles. During this meeting it is also important for the leader to ask intuitive questions, so they are aware of the things that motivates their nurse employees to continue being a nurse every day to help others. Remind them why they started this career, so even through the negative days they resort back to the positive reasons why they started their nursing career.
In today’s recruitment efforts, the candidate pool of nursing talent is getting smaller since nursing schools can’t accommodate the applicants. Even though the schools can’t accommodate the volume of applicants, the nursing programs still need to ensure their selection process is fair in diversity selection as well. Health care organizations also need to focus on out of the box recruitment efforts targeting different populations—specifically, minority nurses. Health care in the United States is seeing a high influx of minority patients. When the number of minority patients increase, so does the demand for minority nurses to care for those patients. It is very important for the team of nurses at an organization to be well-rounded and diversified to care for patients from a variety of cultural backgrounds.
Implementing training programs, leadership engagement, and targeting minority nurse nurses will not only help with recruitment and retention, but also project longevity amongst nurse employees. Nurses need to feel wanted and valued. Nursing is one of the toughest jobs, but when an employer makes them feel respected, appreciated, and gives them the proper tools to be successful, they will be more likely to continue to stay within an organization that supports them wholeheartedly. Every organization needs to focus on these areas to be able to retain their nursing staff and provide the utmost care to their patients every day.
The 57-year-old woman is standing in the hall outside of the exam room. She is agitated. “I’m waiting for the doctor. I’m freezing! My back is killing me!” I note she is pale, unable to stand still, and has a sheen of perspiration on her forehead. She is in withdrawal. I get her a blanket and ask her to wait in her room. The pain clinic nurse is downstairs at the pharmacy getting the patient’s prescription for Suboxone for induction. Induction is the process of starting the patient on medication and finetuning the dose.
An hour later the patient is back in the hall calling me, “Thanks for the blanket!” She is smiling. Her color is back. She is clear eyed, calm, and collected. What happened? Suboxone. Suboxone is a combination of buprenorphine and naloxone that is used to treat opioid addiction. Buprenorphine is a partial agonist of the μ-opioid receptor with a high affinity and low rate of dissociation from the receptor. In English, the buprenorphine molecule sticks to the opioid receptor in the brain, but only partially activates it. Then it stays there for a long time, blocking it from opioids, before dissociating. What this means for the addict is that they get enough opioid receptor activation that they don’t get sick from withdrawal. They can function normally with less of the problematic effects of a full agonist like morphine or heroine.
The addition of naloxone, a
full opioid antagonist (blocker), keeps the Suboxone pills from being crushed and injected. Though naloxone has a strong effect when given parenterally (by injection), its effect when given by mouth is negligible because it is poorly absorbed sublingually. Suboxone disintegrating tablets are given under the tongue.
So, what is this wonder drug all about? In 2000, federal legislation (Drug Addiction Treatment Act of 2000) made office-based treatment of narcotic addiction with schedule III-V drugs legal. Until then, the only option for addicts was abstinence-based treatment or methadone clinics. The ever-increasing rates of drug overdose deaths in the United States showed this was not working. At first, only MDs specially approved by the Department of Health and Human Services could prescribe medications to treat addiction. In 2016, President Obama signed the Comprehensive Addiction and Recovery Act allowing nurse practitioners and physicians assistants to prescribe schedule III-V drugs for the treatment of addiction. Previously, they could prescribe these medications to treat pain but not to treat addiction.
What does this mean for the addict? For starters, Suboxone and similar drugs are now more widely available. Until recently, the only way for a heroin addict to keep from getting withdrawal sickness was to use more heroine. These patients were considered toxic to regular doctors because their disease lead to ever-increasing doses, seeking medications from multiple providers, decreasing levels of health, and ultimately death. Now that there is an option other than going cold turkey, the addict without some kind of pain diagnosis can get access to health care whereas before they would avoid it because of the stigma of being an addict. Because Suboxone is a partial agonist with high affinity to the μ-opioid receptor, it decreases the ‘high’ if the patient continues to use narcotics causing the patient to lose interest. It offers the benefit of allowing the addict to function in life, decreases the likelihood of death from respiratory depression, and increases the quality of life because there is no need for the addict to ride the wheel of withdrawal—drug seeking, using, running out, and then seeking again to the exclusion of every joy of life.
What happens when a person starts buprenorphine? After a largish battery of tests, the prospective recovering addict will be asked to abstain from narcotics before induction to Suboxone. How long before the first dose the addict has to abstain depends on the person’s addiction. Longer acting drugs like methadone could be 24 hours. Shorter acting drugs like morphine could be as little as six hours. The person should be in the early stages of withdrawal. The reason for this is the “partial” part of partial agonist. The buprenorphine molecule will muscle other narcotics off the receptor site where it was fully activating the receptor. Now, the higher affinity buprenorphine is sitting there doing half the work that the heroine was doing and this leads to symptoms of withdrawal. Giving a person a drug that puts them immediately into withdrawal will turn them off to it completely. You won’t see that person again. Higher success rates are tied with higher levels of symptoms of withdrawal before induction. Now instead of precipitated withdrawal, the person has relief from symptoms of withdrawal even if they are not getting high.
A person who has been successfully inducted to Suboxone therapy will find almost immediate relief. The terrible body aches, muscle pain, abdominal pain, depression, diarrhea, and cravings evaporate. Our patient might just have found a new way to live, free from the constant need to find more narcotics. She can focus on her life instead of her disease. Most of the clinic patients have jobs. They want desperately to be productive members of society for themselves and for their families. Buprenorphine therapy coupled with lifestyle interventions provided by mental health professionals, self-help groups like Narcotics Anonymous, and patient-initiated interventions (like taking a class or going back to school) are part of the success story of a growing number of recovering addicts.
What’s it like to come off Suboxone? Eh, probably a lot like getting off heroine. Same withdrawal profile or pretty close. Patients wanting to get off all narcotics, including Suboxone, can be weaned off gradually depending on their desired treatment goals. Someone facing a jail sentence or travel overseas that needs to detox from opioids quickly may be on a tapered dose of Suboxone for just a few days or weeks. Other people may decide that the burden of staying on Suboxone is worth not having to go through withdrawal and choose to stay on a maintenance dose for the rest of their life. The addiction specialist will help guide the patient through the decision process. Many patients decide to stay on the medication as a hedge against relapse since buprenorphine has a higher affinity for opioid receptors than street drugs. This coupled with the very slow rate of dissociation means that a person would have to stop the buprenorphine well in advance of restarting heroine or other opioid in order to get high.
What does this mean for health care? For one, at least some addicts who eschewed health care in the past can now get treatment for this disease. At some point, most addicts will desire to get off narcotics. Having a real treatment option available instead of a far-away methadone clinic or withdrawal will work to drive these patients into recovery. Another thing is that it’s possible that some of the stigma of addiction will be lifted, at least slowly, as treatment becomes available and success stories become commonplace. As the DEA and FDA work to get a handle on the 70,000 overdose deaths per year by educating doctors and enforcing distribution laws, these drugs will become harder to get. During the 12 months prior to July 2017, overdose deaths fell in 14 states for the first time during the opioid epidemic, according to the Centers for Disease Control and Prevention. In the rest of the nation, at least the numbers have leveled off. Greater access to Narcan (brand name of naloxone, one of the drugs in Suboxone), and more treatment options for addicts will hopefully drive these numbers lower over time. It’s not time to celebrate, but at least there is a glimmer of hope. The priority is to keep addicts alive until they can (or they are ready to) get treatment for their disease.
What is diversity? According to the Oxford English Dictionary, it is “the condition of being diverse, different, or varied; difference, unlikeness.” This simplistic definition of diversity does not assign any judgment or negative connotation to any of the words used to define it. However, the word “diversity” evokes multidimensional judgements, reactions, ideas, emotions, and actions, some of which could have adverse social and health consequences for generations of individuals in the United States.
Nursing, as the largest health care workforce in the United States with over 3 million nurses, is well positioned to champion diversity efforts. In 2010, the Institute of Medicine (IOM) published a landmark report, The Future of Nursing: Leading Change, Advancing Health. In this report, the IOM indicated that the nursing profession was not diverse to care for diverse populations across the lifespan. The IOM recommended that a diversity agenda be promoted, especially with increasing the diversity of nursing students. In partnership with AARP, the Robert Wood Johnson Foundation (RWJF) launched a campaign to implement the IOM recommendations from its 2010 report. Subsequently, commissioned by the RWJF, the IOM evaluated the state of affairs regarding these recommendations. In 2015, another report, Assessing Progress on the Institute of Medicine Report The Future of Nursing, was published. In this report, the IOM specified that nursing has improved on the recommendation to diverse the nursing workforce. Nonetheless, there remain gaps that must be addressed to meet the diversity goal for the nursing profession. Consequently, the new recommendation for nursing is that diversity must continue to be a priority that is paralleled with a series of actions to promote it. Before nursing can accomplish this noble goal, there should be a well-vetted strategic plan on diversity and inclusion in all nursing programs, schools, and colleges in the United States. Students, faculty, and staff must be an integral part of the dialogue to promote diversity within the nursing profession.
At the University of Florida College of Nursing (CON), we held our inaugural “Diversity and Inclusive Excellence” workshop in December 2015. This two-day workshop was designed for staff and faculty. As a member of the Diversity taskforce, I collaborated with the other taskforce members to invite G. Rumay Alexander, EdD, RN, FAAN, to lead the CON on this discussion. Alexander is director of the Office of Inclusive Excellence in the School of Nursing at the University of North Carolina at Chapel Hill, a nationally known expert with vast knowledge and expertise on diversity and inclusive excellence, and president-elect of the National League for Nursing.
During the early morning hours of December 3, 2015, my individual lesson on the topic began with Alexander as I had breakfast with her. My antenna on the topic sharpened following our conversation. After introducing her to my fellow Diversity Taskforce members, I hurried to pack my car and return to the CON to proceed with the plans of the day. I noticed the dean, Anna McDaniel, PhD, RN, FAAN, from a distance. I hurried up to keep her pace. “Good morning, Dean,” I greeted in my usual manner. McDaniel responded with a broad smile and a twinkle in her eyes that I perfectly understood. I surmised that McDaniel had finally accepted the fact that I love referring to her as the “Dean.” We conversed as we headed to the CON and into the elevator. I noticed the necklace McDaniel wore. The costume necklace had different shapes, colors, sizes, lengths, and mosaic designs. They were
audaciously woven, yet unintimidating;
different, yet complementary;
individually, unassuming — yet, together, a paragon of beauty, inviting;
all held by a perfectly thin strand, yet unbreakable.
“That’s a beautiful necklace,” I uttered. “It belonged to my mother, who died twelve years ago,” McDaniel shared. “Each bead came from a different country. I have a brochure that provides a description of each bead, including the country of origin and its material composition.” Then, McDaniel voiced the word that gladdened my heart. “I wore this necklace today because it’s appropriate to celebrate diversity, the topic of the CON workshop.”
McDaniel had appointed the Diversity Taskforce and provided us with her full support. But, the fact that she actually thought of and adorned herself with a necklace that I now coined as a “diversity necklace” to celebrate the CON inaugural diversity workshop was admirable to me.
Someone not sensitive to the current diversity concerns around the United States, and the racial unrest related to such matters, may not appreciate my exhilaration upon hearing the history of the necklace. At issue is that, in several communities around the United States, numerous individuals are thoughtless about the devastating effects of antidiversity rhetorics and actions on the lives of its victims. Many may not realize that any action, whether good or evil, begins in the mind. Conversely, any work to combat uncelebrated diversity and exclusivity must begin in the mind. When people think about and proactively perform small acts, such as expressing recognition of diversity through a piece of jewelry or other special actions to celebrate diversity, it goes a long way. It could change the thought process from exclusion to inclusion. When people are attentive to their behaviors and understand the detrimental effects their actions could have on other human beings, things might change for the better. I believe that, as a nation, we must check the poisonous thoughts that percolate in our minds and subsequently manifest in forms of antidiversity rhetorics and behaviors, unacceptance, and racism. Confronting monstrous suggestions in the mind is the first step that many of us need to take to begin to challenge the subtle and insidious systemic diversity-aversion and exclusion in the United States.
As I thought about this issue of diversity and the role that nursing can play to eliminate it, I reminisced about how the imperfections of people categorized within the social construction of race stimulate antidiversity and anti-inclusive sentiments and movements. I wondered how nursing can care for these individuals, many of whom are marred with scars of history. My poem, “The Color of Justice,” captures my perceptions of the undeniable genesis of these historical blemishes that shockingly remain, overtly or covertly, as status quo in various parts of this country.
The Color of Justice
What color is justice?
Absorbing pain, insults, and lashes
Ancestors packed shoulder-to-shoulder, hip-to-hip,
chained like fire woods
Bones of the feeble lie un-mourned in ocean deep
across the Atlantic
Their sweat built the wealth in the new world, but
crumps have become their portions
This name sound like them, we have filled the position,
they need to go away
Low-hanging pants, cove-hopping birds,
gun-brandishing bunch
We cannot deal with the anger, we are better off
with the accent, intra-color battle ignited
Round them up, throw away the key, population control
Babes on the breast, mama and grandmamma, sitting
on the front porch pondering about the next check
Hair tightly woven, fried, or twisted, nails freshly manicured, next bun in the oven
The fortunate may triumph at the end, treacherous roads treaded, stress claims the wounded body after all
That they survive is still a mystery that ought to win
them a trophy
Who are they?
What color is justice?
Reflecting heat, demanding respect, crushing heads
Rolled into the new world in Mayflower boasting of
prostitutes, thieves, and prodigal sons
Raised arms against raised tea taxes, won freedom
but deny it to another
Melanin deficient hue suggest superiority
Blood by blood, noose on hand, destroyed a generation,
eye un-batting
Deeds done in the name of God, He must be weeping
Damages proudly scattered in museums, we pay to
relive the tragedy
Privileges left and right on the backs of the poor
Man in bow tie, lady in heels, rear the children, your lavatory in the rear
Own your history, mend your ways, teach your babes right
Who are they?
What color is justice?
Broad face, warm hue, and welcoming gesture
Land is supreme and cares for the offspring
Infected with strange diseases, killed with gun powder, survivors kept in special places devoid of opportunities
Culture deconstructed, the sacred used as mascots
Surviving by balancing mind, body, and spirit, harmony
in the land is their mantra
Not many left but their spirit is strong
The land beckons for their touch, to purge its roots of deadened souls
What does the Unites States’ constitution say about them?
Who are they?
What color is justice?
Messiah has come, awaiting messiah, there is no messiah
We profess peace, spiritual path is the way
Whose belief is superior?
When six feet under, belief quenches, but tainted
souls still suffer
Where are their senses?
Who are they?
What color is justice?
Light? Energy? God?
Penetrates Black, White, Red hue, religious, non-religious
Building block of things created
Revitalizes without questioning, unites all things created
Shines for Black, White, and Red hue, religious and
non-religious
Knows no foolishness but shines for fools
Knows no discrimination but supports the life of discriminators
Invites reconciliation until judgement day
Come unto me Black, White, and Red hue, religious,
non-religious
My light is your strength, unity, and peace
One may wonder how a nurse who is an advocate for a diverse, inclusive, and just world could pen “The Color of Justice.” This poem reflects my dual perceptions as a black woman and a nurse, of how the historical racial unrest that has plagued the United States for centuries has been subtly perpetuated even today. But, they ought not have continued, had the United States paid real attention and reconciled both the apparent and undercurrent narratives of this poem after the abolition of Jim Crow laws. As a black woman, I think that the first relevant question ought to be: How do individuals from diverse backgrounds interpret their historical or lived experiences in the United States? I encourage each one of us to answer this question individually or as a family, church, academic institution, or financial organization. I assert that there must be a recognition and acceptance of the different dimensions of diversity of thoughts, ideas, and experiences. This recognition must be matched with “courageous dialogue” on diversity and inclusion. In addition, there have to be concrete and measurable action plans for allocating resources to implement iterative strategies to address identified diversity concerns. This exercise could be so powerful that diversity and inclusion become strengths and not detriments to our collective humanity.
As a nurse, I think the second pertinent question must be: What role can nursing play to mitigate the adverse generational effects of antidiversity and anti-inclusivity experiences on marginalized and excluded individuals? I contend that, in order for nursing to be professionally and culturally relevant in the future and to continue to have the public trust as a caring discipline, we must identify ways to champion the diversity and inclusive excellence agenda. There should be constant and mandated training on diversity for university staff and faculty, with measurable outcomes. Nursing as a profession should develop a curriculum with a diversity and inclusion plan threaded throughout it. One approach to operationalize this suggestion is to equip nursing students with skills necessary to be culturally competent, diversity-savvy, and inclusive-perceptive in order to encourage these values in their work settings. Patients and clients at the receiving end of compassionate, culturally competent care infused with the spirit of diversity and inclusiveness should remember the feelings associated with that care, and hopefully pay it forward. Slowly, the culture of superiority and nontolerance directed toward individuals from diverse backgrounds could dissipate and a new world facilitated by nursing and inhabited by truly compassionate and empathetic humans would emerge.
Nursing students are the future of the nursing profession. Therefore, nursing must constantly remind students that antidiversity and anti-inclusion rhetorics and behaviors, historically and contemporary, breed racism in the United States. They should also learn to celebrate how much improvement we have made as a profession. But, recognize that diversity work is lifelong. The juxtaposition of the history of racism in the United States with the improvements made toward eliminating it is useful for at least two reasons: The contrast provides the space for constructive discourses and opportunities to develop positive avenues for endorsing diversity, and it allows for future and ongoing actions to completely obliterate racism heralded by antidiversity and anti-inclusive beliefs in the United States. Consequently, bead by bead—though diverse in shapes, colors, sizes, lengths, mosaic designs, and historical origins—we can hang unbreakably strong on the perfect strand of humanity, which unites us as “one Nation under God.”