Pamela Meharry, PhD, CNM, RN, first arrived in Rwanda in 2015, part of an ambitious initiative to train the healthcare workforce in the post-genocide country in east Africa.
Pamela Meharry, PhD, CNM, RN
She was there to co-teach in the newly created Bachelor of Science in midwifery program at the University of Rwanda.
But in a short time, Meharry saw a need for more than a bachelor’s program, envisioning an advanced degree where midwifery leaders could be cultivated on Rwandan soil.
“The midwives I taught with had either gone abroad to Australia, Canada, Scotland, South Africa, or Uganda for their midwifery master’s degree, or completed a master’s program in another discipline,” she says. “When I first started talking about a master’s in midwifery, [my colleagues] said, ‘you’ll have 50 people signed up on day one to join that class. So many midwives wanted to do it, but there was no program.”
Following years of planning with other stakeholders, Meharry’ s vision will become a reality in April, when the inaugural class of students will begin in the Master of Science in midwifery program at the University of Rwanda.
Reducing mortality rates
The University of Illinois Chicago (UIC) School of Nursing hired Meharry – who was working in Connecticut as a midwife and instructor – to travel to Rwanda under the banner of the Human Resources for Health Program, the largest U.S. academic global health consortium to date.
Meharry was paired with the head of the midwifery department and co-taught bachelor’s degree and master’s degree students in the neonatal nursing program, but she observed that a master’s in midwifery program was also sorely needed to develop teachers and leaders.
There were eight other masters’ programs in the School of Nursing and Midwifery at the University of Rwanda, though none that specialized in midwifery or women’s health.
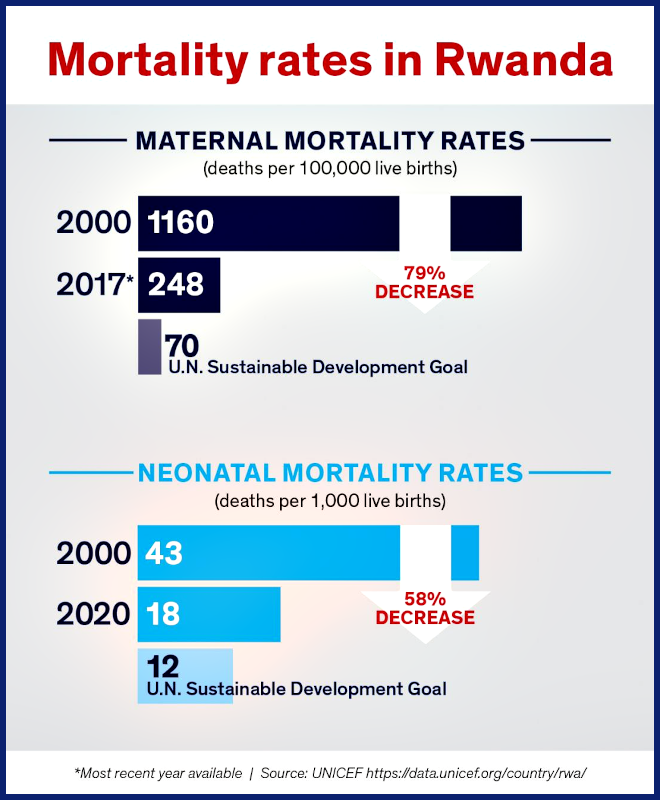
She adds that midwives are considered vital assets in the global effort to lower maternal and infant mortality rates. In Rwanda, those rates have decreased significantly over the last 20 years, but there is more work to be done to reach U.N. Sustainable Development Goals by the benchmark year of 2030, she says.
UIC Nursing shares curriculum
With permission from her Rwandan department head to begin pulling together a curriculum, Meharry contacted UIC Nursing’s then-associate dean for global health Linda McCreary, PhD ’00, MS ’93, BSN ’73, RN, FAAN, and nurse-midwifery program director Carrie Klima, PhD, MS ’86, CNM, FACNM, FAAN. Those colleagues shared with her the UIC DNP nurse-midwifery curriculum, giving her a strong basis from which to develop a curriculum appropriate for a new master’s program at the University of Rwanda.
Meharry was involved in curriculum development even as she conducted a Fulbright teaching and research grant in Zimbabwe in 2019 and 2020. The new master’s program was approved in November 2021.
Meharry says this will open doors for midwives.
“At the master’s level, well-trained midwives [can] assume a leadership role in training midwives, increasing competencies and critical decision-making skills, stimulating research and publications, and integrating more evidence-based practice into health facilities,” Meharry says.
Developing research and study abroad opportunities
During her seven years in Africa, Meharry has also played a vital role in mentoring student researchers, helping 27 nursing master’s graduates publish articles in issues of the Rwandan Journal of Medicine and Health Science.
These publications have become a labor of love and significantly enhance the graduates’ prospects of promotion and PhD studies,” Meharry says. “We now have six graduates in the new PhD program, and they [recently] presented their doctoral proposals to the faculty for review.”
Meharry also helped the head of the midwifery department to publish her master’s research and is now co-supervising her PhD research.
Originally from New Zealand, Meharry says she loves Rwanda’s temperate climate and open spaces. However, what keeps her there is the opportunity to help build programs and develop a research-rich environment, which she finds very rewarding.
She’s hoping to pass that enthusiasm on to UIC Nursing students by serving as faculty director for a month-long Rwanda study abroad program in July 2022 — Global Maternal and Child Health in Rwanda – the first maternal and child health course offered by the UIC Study Abroad Office.
You may not hear much about the “frontier” these days, but the Frontier School of Midwifery and Family Nursing in Hyden, Kentucky, is alive and well. The school recently received a $1.03 million grant to support students with an associate degree in nursing complete their M.S.N. It’s a one-year bridge program conducted entirely online, followed by studies in a clinical specialty track.
The award comes from the Health Resources and Services Administration, a federal agency devoted to improving health care access among the uninsured, isolated, and medically vulnerable. With this new grant money, the Frontier School can hire the necessary faculty to run the program and improve its recruitment and retention capabilities. In particular, they hope to increase the numbers of rural and minority students in the A.D.N.-M.S.N. program.
At the Frontier School, students can earn their M.S.N. with certifications in nurse midwifery, family nurse practitioner, and women’s health care nurse practitioner, or a Doctor of Nursing Practice, all via distance learning. The School hopes to enroll 75% of its bridge program students from rural areas, so they may return and practice where residents are typically medically underserved.
The Frontier Nursing University in Hyden, Kentucky, is launching a new campaign to increase diversity in nursing. The PRIDE Program has a good acronym for an even better cause: Promoting Recruitment and Retention to Increase Diversity in Nurse-Midwifery and Nurse Practitioner Education.
“The ultimate goal of the PRIDE program is to recruit and retain qualified underrepresented students in our graduate school of nursing who will meet the health care demands of an increasingly diverse population,” the school says. They kicked off the campaign this past June with its first annual Diversity Impact weekend. The tight-knit, intimate event of 16 students held diversity forums and networking opportunities. They discussed and debated issues such as “Resources on Racial Disparities,” “Surviving Distance Education,” and “What’s Race Got To Do With It: A Courageous Conversation About Race.”
The weekend also included presentations regarding cultural beliefs and health conditions specific to certain demographics—even a potluck dinner of recipes from different cultures. All visiting students were given a $500 travel stipend, funded by a grant from the Health Resources and Services Administration (HRSA). The Frontier University (formerly Frontier School of Midwifery and Family Nursing) has been educating nurse practitioners and nurse midwives to work in rural and otherwise medically underserved communities for 70 years. For more information regarding the PRIDE initiative and a summary of the weekend’s events, visit www.frontier.edu/diversityimpact.
Midwifery is a profession that is as at least as old as the Bible. In Exodus 1:15-21, Shiphrah and Puah were midwives who refused the Egyptian Pharaoh’s order to kill all newborn Hebrew males. Today, midwives continue to provide care to women who, for a variety of reasons, are vulnerable and in need. They care for women of all ages, races, ethnicities, sexual orientations, socioeconomic groups and educational backgrounds.
Certified nurse-midwives (CNMs) are educated in the disciplines of nursing and midwifery, usually at the graduate level, and have been nationally board certified through the American Midwifery Certification Board. They are trained to work in a variety of practice settings, including high-volume hospitals, small community hospitals, birth centers, health departments and clinics, as well as the home birth setting. CNMs provide care for women from puberty through menopause. The many services they provide include nurturing pregnant women through childbirth, primary care, pre-conception counseling, family planning, menopausal care and general women’s health care. In addition, they are trained to care for newborns during the first month of life.
Midwifery has had a long and significant history in the African American community. Yet despite this rich legacy, black nurses—as well as other nurses of color—continue to be substantially underrepresented in today’s nurse-midwife workforce.
History of African American Midwives
In the early 17th century, the slave trade brought many African slaves to America. Among them were women who brought generations of knowledge about childbirth to the American culture. These African slave women, along with immigrant European midwives, made significant contributions to midwifery in the early years of the United States’ existence.1 African midwives proudly handed down the skill of midwifery from mother to daughter, in an apprenticeship model, while keeping strong ties to African-based rituals and customs.2
In the years following emancipation, African American women who entered the midwifery profession often did so out of a spiritual calling. These midwives, often referred to as “granny midwives,” were matriarchs within their communities. They served as advocates, healers and liaisons between the health care system and their communities.1
By the turn of the 20th century, only 50% of all American women giving birth were attended by midwives. However, most immigrant women, African Americans and other poor women continued to almost always be cared for by a midwife. This difference in care was attributed to the inability of these women to pay physician fees, the notoriously poor care provided at segregated black hospitals and moral opposition by many women to male birth attendants.3
Today’s African American CNMs continue the legacy of the post-emancipation midwives by continuing to bring quality care to women and newborns whose need is greatest. They serve low-income families, Medicaid recipients, teen mothers and the uninsured. The Centers for Disease Control and Prevention (CDC) reported in 1998 that CNMs, more than physicians, served a greater proportion of women who were at higher risk for poor birth outcomes. These included African Americans, Native Americans, teenagers, unmarried women and those with less than a high school education.4
A Need for Diversity
In the 21st century, with the U.S. population reaching unprecedented levels of racial, ethnic and cultural diversity, nurse-midwives continue to make a consistently positive contribution to the health outcomes of women from vulnerable populations. Because of the tremendous need for health care professionals who share common bonds with the patients they treat, minority nurses can offer a wealth of cultural knowledge when providing care to patients in communities of color.
Although midwives provide care for many minority women in America today, the midwifery profession is not diverse. There is a lack of minority nurse-midwifery students entering the field, as well as a lack of minority instructors and researchers. In 2003, the American College of Nurse-Midwives (ACNM) reported that less than 4% of CNMs identified themselves as African American, approximately 1% were of Asian descent and less than 1% identified themselves as Hispanic. Furthermore, less than 1% of CNMs were men.5
In contrast, according to the American Association of Colleges of Nursing (AACN), the student population currently enrolled in general MSN degree programs is 11.3% African American, nearly 5% Hispanic, 6% Asian American and 8.9% male.
In the fall of 2006, AACN member nursing programs reported that nearly a quarter of their students (24.8%) were from racial or ethnic minority groups.6 However, nurses of color account for less than 10% of all baccalaureate and graduate school nursing faculty.7
Although these statistics suggest that there is at least a slight increase in the number of minority students entering the field of nursing, there is still a disproportionately low number of candidates from these ethnic groups entering CNM programs.
Choosing a Nurse-Midwifery Program
There are many different educational options available to minority nurses who are interested in becoming certified nurse-midwives. BSN-prepared registered nurses (RNs) can apply directly to a midwifery graduate program. Some graduate programs also allow RNs with associate’s degrees to pursue a degree in nurse midwifery. There are also accelerated “fast-track” education programs that offer students the opportunity to become RNs and then CNMs, earning a graduate degree in approximately three years of full-time study. Like generic “master’s entry” nursing programs, these programs are typically designed for students who have obtained a four-year degree in a discipline other than nursing—such as a BA in public health—yet have completed all the traditional prerequisites for nursing school.
ACNM has a Web site that enables prospective students to explore available nurse-midwifery education programs across the United States. Instruction methods vary from 100% distance-learning programs to 100% on-campus programs. Still other institutions offer CNM programs that are a combination of both online and classroom learning.
To find the program that’s the best fit for you, it’s essential to investigate all options. When considering schools, you must be savvy and proactive. Visit the school’s Web site, talk with admission counselors and with students currently enrolled in a midwifery program. After you have narrowed your search, begin to consider factors such as cost, program size and the reputation of the program, as well as the school’s commitment to diversity and providing a supportive environment for minority students.
When examining the cost of a program, be mindful of potential hidden costs such as books, activity fees, health insurance and travel expenses for clinical rotations. If you think that the financial expenditure is not within your means, search for scholarship opportunities and other possible financial assistance within the schools of your choice. Some schools may have internal scholarships and awards based on criteria such as grades, academic performance and financial need. You should also explore external scholarships from professional organizations such as ACNM or the Association of Women’s Health, Obstetric and Neonatal Nurses (AWOHNN).
Other financial questions to consider when choosing a program may include the following: Are student employment opportunities available? Are there any tuition payment opportunities at an affiliated hospital? Look into whether there are any health care organizations or practices that might be willing to support you financially through a CNM program in exchange for a commitment to work for that organization after you graduate.
The size of a nurse-midwifery program is also important. Factors to consider include: Is the class large enough to encourage diversity of issues and perspectives? Is the program large enough that students can find other students whom they can identify with? How many faculty members are there? Do students seem to know faculty members well and have positive things to say about their classroom experience? How well does the faculty know the students? Are faculty members accessible to students?
Trickera Sims, MSPH, RN
In other words, the class size will impact your ability to interact with fellow students and faculty, and to establish professional relationships. Ask to meet with current or past students to gain insight and knowledge about student life. It may be beneficial to observe a class session to get a first-hand look at faculty-student interaction. Meet with at least one of the faculty members during a campus visit to discuss instructors’ expectations and involvement with students.
The reputation of a CNM program is a valuable screening tool in selecting a potential school and is directly related to the students’ success rate on the national board certification exam. Investigate such questions as: What is the pass rate on the national certification exam? Are there adequate numbers of faculty and administrative staff employed in the program? Is the program new or well established? Each of these questions may help you prioritize programs and identify the best school for you. However, it is imperative to know the pass rate because it is a reliable indication of overall graduate preparedness.
Finally, examine the school’s commitment to providing a welcoming, supportive environment for students of color and other students from underrepresented populations. Find out whether there are active organizations and programs geared towards supporting minority students during their matriculation. Is faculty mentorship available? If so, how many students does an individual faculty member mentor? How many minority instructors are in the program or in the school? Is there an active recruitment campaign to increase diversity of both students and faculty? What resources are in place to recruit and retain minority students? Are there other minority students who are willing to talk to you about their experience?
Once you have narrowed your search, it is important to visit the campus. Even if the number of minority students is few, you can still get a feel for the school’s culture and whether there are students with whom you have other things in common—e.g., students from your same geographical area, students who are parents, working students. A wealth of knowledge and information can be obtained from talking to current students, such as their perceptions of support from faculty and the school, intensity of the class work and the rigors of clinical training.
Additionally, if attending this school will result in relocation, look at the community. What does it offer you and your family? This may include housing, schools, childcare, transportation (including commute considerations), spiritual or organized religious organizations, and job opportunities.
Midwives Make a Difference
Today, as in the past, midwives are on the front lines of providing care to women from all walks of life. Research studies and federal health statistics confirm the positive impact that nurse-midwives make on the lives of women and children. Mothers, babies and entire families lead healthier lives because of the care provided by CNMs.
By making quality health care accessible to women from vulnerable populations who are most at risk for problems during childbirth, nurse-midwives can make a real difference in reducing risks of infant mortality and other health disparities. This is why the health care industry has an undeniable need for more minority CNMs who can relate to the cultural backgrounds of minority patients and provide culturally appropriate care that is sensitive to their needs.
Traveling the road to becoming a nurse-midwife is a journey filled with wonder and excitement. Each day proves to be a challenge and an opportunity to make a difference in the lives of so many. Learning more about this exciting profession and thoroughly researching schools and programs that provide nurse- midwifery training could start you on that journey to a truly rewarding and gratifying career.
References:
1. Robinson, S.A. (1984). “A Historical Development of Midwifery in the Black Community: 1600-1940.” Journal of Nurse-Midwifery, Vol. 29, No. 4, pp. 247-250. br /> 2. Rooks, J.P. (1997). Midwifery and Childbirth in America. Temple University Press.
3. Litoff, J.B. (1982). “The Midwife Throughout History.” Journal of Nurse-Midwifery, Vol. 27, No. 6, pp. 3-11.
4. Centers for Disease Control and Prevention, National Center for Health Statistics (1998). “New Study Shows Lower Mortality Rates for Infants Delivered by Certified Nurse Midwives.” Retrieved from www.cdc.gov/nchs/pressroom/98news/midwife.htm.
5. Schuiling, K.D., Sipe, T.A. and Fullerton, J. (2005). “Findings from the American College of Nurse-Midwives’ Membership Surveys: 2000-2003.” Journal of Midwifery and Women’s Health, Vol. 50, No. 1, pp. 8-15.
6. American Association of Colleges of Nursing (2007). “2007 Annual State of the Schools.”
7. The Sullivan Commission (2004). Missing Persons: Minorities in the Health Professions.
Since 1976, Nivia Nieves Fisch, CNM, has assisted some 2,500 women during the births of their children. Midwifery is a career that she is clearly passionate about and one that brings her great personal satisfaction. “It is not just my profession,” she says. “It is part of who I am.”
As registered nurses with special training in childbirth, CNMs (Certified Nurse-Midwives) provide a wide range of health services for female patients and their families. Fisch, who is of Puerto Rican descent, resides and works in Harlingen, Texas, a town located in the Rio Grande Valley near the Mexican border. She is one of only two nurse-midwives of color working in the valley, she estimates, out of approximately 30 local CNMs. “We are such a small group,” she says of minority midwives in general. “Midwifery itself is small group, but it is growing. Yet, there are still very few nurse-midwives of color.”
That is a trend Fisch would like to see changed. “Patients need to be spoken to in their native languages,” she explains. “It’s important for nurses to know [their patients’] culture. I’m not saying that Caucasian nurses can’t learn that, but people of color feel more comfortable when they see faces that look like their own.”
Fisch works in private practice with Harlingen OB/GYN Associates, which employs four obstetricians as well as one other CNM. Ninety percent of her patients are Mexican American, she estimates. When she first came to Texas as a CNM, she worked at an out-of-home birth center and eventually became its director. “When I came down here to practice, the majority of births were happening at home with traditional midwives,” she says. “That is what people associate with midwifery.”
As these traditional midwives began to age and leave the profession, nurse-midwives stepped into their shoes. “We started to replace them as our profession grew,” Fisch remembers. “It was really easy to attract patients to nurse-midwifery because [traditional midwives] had been here for a long time and were respected by the community.”
A Spiritual Approach
Since Fisch started her private practice in 1983, all of the births she has assisted in have been hospital deliveries. But, she stresses, her philosophy of midwifery sees birth as a natural process. “I don’t consider it an illness at all,” she says. “I consider it a spiritual experience for families. If you harness the energy that a newborn produces in the birth process, you can have a wonderful family event; it can be the bond that holds a family together for years to come. If more people concentrated on that, we would probably have more stable families.”
This philosophy, Fisch continues, is what separates nurse-midwives from obstetricians. “Because the basis of midwifery is family and tradition, we tend to focus more on the family’s spiritual needs,” she explains. Midwives are also concerned with the physical needs of the mother and child, she adds, but the focus is more on support and nurturing instead of medications and interventions. “You are not focused on the technology. You are focused on the patient.”
However, some of the care a midwife provides is the same as what an obstetrician offers. “I tend to perform fewer episiotomies than doctors do, but if it is needed, I can do it,” says Fisch. “And I am ready to move a patient to someone else’s care, if necessary. Midwives know there are limitations to the practice.”
Because midwives emphasize the natural and spiritual aspects of childbirth, their goal when assisting at a delivery is to have a drug-free birth. But, says Fisch, “that can be difficult in a hospital setting because people have developed expectations that modern medicine means no pain.”
This is not the case in every country, though. This spring, Fisch traveled to Honduras to teach life-saving skills as a consultant for the American College of Nurse-Midwives (ACNM)’s Global Health Division. The hospital she visited there had no pain relief medicine available for women giving birth. “Delivering in the hospital was no different than delivering at home, except that you were in a medical environment,” she relates. “Those women did not request pain relief. Unlike Americans, Honduran culture does not think labor should be painless.”
In her own practice, Fisch will use epidurals, albeit rarely. While medication will reduce the pain associated with childbirth, Fisch is quick to point out that it also takes away some of the mother’s control over the birth process. “It can also have potential side effects,” she says. “If things are normal and the patient is not at risk, I don’t think epidurals are the solution for a good birth experience.”
According to H. Frances Hayes-Cushenberry, CNM, MSN, most nurse-midwives would agree with that assessment. “If you practice the true art of midwifery, then you don’t do any intervention,” she says. “You don’t have to use invasive techniques. You are allowed to let the process take place naturally.”
Developing Minority Nurse-Midwives
Hayes-Cushenberry, who is African American, teaches nurse-midwifery at Charles R. Drew University of Medicine and Science (www.cdrewu.edu/) in Los Angeles, a historically black college. Its midwifery program is dedicated to educating minorities and underprivileged students and increasing the number of OB/GYN primary health care providers who work in underserved communities. Hayes-Cushenberry estimates that 70% to 80% of the university’s midwifery graduates work in rural and inner-city areas.
Because of the university’s midwifery program, there are now a number of minority nurse- midwives working in the Los Angeles area, Hayes-Cushenberry reports. But on a national level, the number of minority nurses in the profession is very low, says Anne Richter, CNM, MPH, co-chair of the Safe Mother Initiative, USA (SMI-USA). She points to a recent ACNM survey which found that only 3.8% of the nurse-midwife population is African American, 1.9% is Hispanic, 1% is Asian and 0.4% is Native American. The survey, which polled 5,410 CNMs, was published in the Journal of Midwifery and Women’s Health.
Richter feels the profession clearly needs more minority nurses, particularly African Americans, because minority women tend to have more complications from childbearing than Caucasian women. She cites research indicating that African-American women are four times as likely to die during childbirth as Caucasians, and that Hispanic women are 1.6 times more likely than non-Hispanic white women to die from pregnancy-related causes.
Another major issue minority mothers face is lack of access to health care services. According to SMI-USA, Hispanic women are 2.5 times more likely to be uninsured than Caucasian women; African-American women are almost twice as likely to not have insurance. African-American and Hispanic women are also more likely to receive late or no prenatal care.
Culturally Competent Midwifery
Still another barrier expectant minority women can face is a lack of cultural and linguistic competence from their health care providers. Studies have shown that when African-American women receive care from providers who are not African-American, the level of communication suffers, Richter says. “Nurse- midwives spend a lot of time listening to their patients,” she adds. “If we could get more nurses of color educated as midwives, it would be a wonderful opportunity for them to empower minority women to reach out and get prenatal health services.”
The American College of Nurse-Midwives is attempting to address such issues through its Midwives of Color Committee. “Our goal is to heighten awareness within the ACNM of the health issues that impact minority populations and to create a supportive environment for student nurse-midwives of color,” says Victoria Fletcher, RN, CNM, MSN, the committee chair. For example, ACNM has a mentoring program that matches minority student nurse-midwives with practicing nurse-midwives of color.
The committee has also provided input to the U.S. Department of Health and Human Services’ Office of Minority Health, which is in the process of drafting recommended national standards for providing culturally and linguistically appropriate health care services (CLAS). Such guidelines have been lacking in the past, says Fletcher, who is African American, because “our nation’s health care system is based on a Western and European model. It wasn’t set up to be inclusive of different races and ethnicities.”
Depending on where they work, part of the cultural competency challenge for nurse-midwives is being able to go beyond just looking at the physical aspect of a patient’s care. “[The patients] may come in once a month and the rest of the time they are living in situations that we don’t get involved with or don’t think of getting involved with,” Fletcher explains. “You may not know that a patient is living in a place without electricity or heat, or that she may not be getting adequate nutrition. Nurse-midwives need to broaden their perspective and deal with some of those issues if we are to ultimately make a difference in reducing maternal health disparities.”
Many health problems have a strong socioeconomic component, Fletcher adds. “What’s missing [in underserved minority communities] is patients who feel supported and who have the education they need to maintain their health,” she says. “Nurse-midwives are trained not only to care for patients based on a symptom or a disease but also to consider them as individuals and to promote health by educating them.”
A Lifetime of Care
The role of midwives often extends well beyond working with pregnant women. “Nurse-midwifery is a versatile profession,” Fletcher emphasizes. “I think people would be surprised to see the continuity of care midwives provide in most settings. We work with women not only through their childbearing years, but throughout their entire life cycles. Pre-menopausal, post-menopausal and even elderly women can be cared for by nurse-midwives.”
While some nurse-midwives choose to limit their practice to a certain portion of this life cycle, their educational training prepares them to work with women at all stages of life. Fletcher’s own practice, for example, does not focus on maternal health. She works for the Bremerton-Kitsap County Health District near Tacoma, Wash., in a clinic that specializes in family planning and sexually transmitted diseases. “I focus more on women’s health issues,” she says. “About 60% of the patients I see are teen-agers.”
There are other things nurses might be surprised to find out about midwifery as well. “I think many nurses feel that going back to school [to learn midwifery] would be very difficult. In reality, it is no more difficult than a regular RN nursing program,” Fletcher asserts. She strongly encourages other nurses of color to look into midwifery careers: “I think they would find this to be a very rewarding profession, and one in which they are definitely needed.”
Fisch feels the rewards of her work every day in her Rio Grande Valley community. “[Because of my job,] I have lots of friends and lots of godchildren,” she says. “My car can stall anywhere in the county, or even the next county, and I wouldn’t be out there for more than five minutes without someone stopping and helping me out. I feel loved by my community. I have a feeling of self-esteem and self-respect that is incredible. I don’t think many people can say that.”
For More Information
Over the past 10 years, the number of Certified Nurse-Midwives (CNMs) has risen steadily, with approximately 400 new CNMs certified in the nation each year. The American College of Nurse- Midwives (ACNM) Certification Council administers the national examination for CNM certification.
To be eligible to sit for the exam, a midwifery student must graduate from an educational program accredited by the ACNM. There are currently 47 such programs offered in the United States.
The ACNM has a membership of approximately 7,000, of which some 5,700 are in clinical practice.
To find out more about nurse-midwifery, contact:
The American College of Nurse-Midwives
818 Connecticut Avenue, N.W., Suite 900
Washington, DC 20006
Phone: (202) 728-9860
Fax: (202) 728-9897
Email: [email protected]
www.midwife.org
The ACNM Web site has information about accredited midwifery programs, licensing, state laws and regulations affecting midwifery, job openings, scholarship opportunities, fellowships and awards, and more.
See Our Champions of Nursing Diversity
Sign up now to get your free digital subscription to Minority Nurse