So, you are thinking about completing your Master’s degree. You may be just graduating with your bachelor’s, established in your career, seeking career advancement, or an overall career change. You should commend yourself wherever you currently are in your professional journey. Graduate school is essential for career progression and as daunting as the challenge may be it is feasible and worthwhile. However, there are certain things that I wish I had known previously to enrolling in my first graduate courses that would have saved me a ton of grief on this grad school journey.
Learn the APA Manual
Do you briefly remember being introduced to this in your undergraduate English and Research classes? You know, the blue book that you couldn’t wait to toss as soon as you completed those courses! Well, don’t get too excited and toss that manual out just yet. The APA manual will be your bible at the graduate level. It is best to not only familiarize yourself with it but read it cover to cover. In all seriousness, there will be no mercy for APA formatting issues at the graduate level, and failure to comply will hinder your ability to graduate. Let’s be honest; graduate school is very expensive so do not lose points over APA errors and get your bang for your bucks when it’s time to cash in on that top G.P.A.
Proofread
Grad school will push your writing capabilities to the maximum. When I first started, I went in under the false pretenses that I was a decent writer. After all, my highest scores were always in English and Language Arts. However, never underestimate the power of proofreading your document, or having someone else review it. It is important to remember that you are not supposed to be writing as if you are talking in scholarly writing. Read every single thing you submit out loud at least two times before turning it in. You will be surprised at some errors you will find in your documents once you hear it out loud. I swear by Owlet Purdue, Grammarly, and PERRLA to assist with the completion of my papers.
Don’t Break
One of the biggest mistakes that I made during my Grad school journey was “taking a break”. Apparently, life happens to everybody, but if you can help it, you should stay on the course to graduate on time. While taking a leave of absence is certainly an option, there are some universities have a time limit on the amount of time you can spend on the completion of your master’s degree. Taking a leave of absence sounds a nice break until you return and you are under even more pressure to complete your degree. Stay on track and graduate on time. Put yourself out of grad school misery. Try not to prolong it.
Find Balance
My zodiac sign of a Libra makes finding balance very high on my priority list. Regardless of your sign, it is essential to find a way to balance everything you have going on in life. Many of us are career focused, have spouses or partners, children, and community obligations. There are going to be some times that you will simply have to say no to others as well as avoid taking on too many additional duties. You have to be able to take care of yourself before you can take care of others. Do not feel guilty about taking a step back or going on a much need hiatus to keep everything together. Remember that this is temporary, and there will always be opportunities to restock your plate once you have graduated.
Cost vs. Reputation
This has been an ongoing debate for such a long time. I will give you my honest opinion and say that it is best to go for value in regards to selecting a school to attend. There is absolutely nothing wrong with investing yourself, but please do not break the bank along the way. Try your very best to avoid debt, save up, and develop a reasonable budget that you can use to finance your educational goals. If you are shelling out a ton of money, ensure that the institution has a reputation that fits your tuition bill. Student loan debt is a serious problem. Remember that you will need to pay that money back, and if this degree does not make a high paying job seem promising to you it may be necessary to scale back. Remember, grad school isn’t cheap!
Wrapping it All Up
I hope that you avoid the pitfalls that I incurred during my grad school journey and that these tips will help ease you in your transition and prepare you for entry into grad school. A graduate degree is totally obtainable; it’s just a different academic dynamic. I’ll see you on the other side!
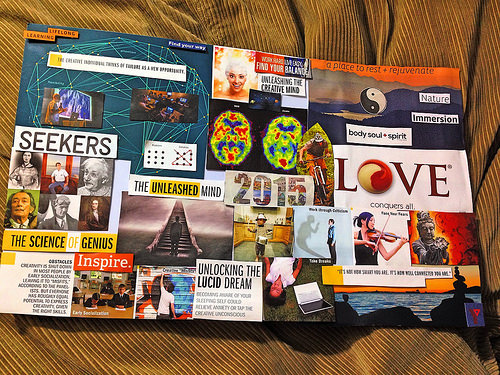
Vision boards are an excellent way to visualize your best life, goals, and dreams. Vision boards are a creative way to generate a visual of the things that you want to see manifested in your life, and a way to provide yourself a daily reminder of why you work so hard, and what your outcome will be. Creating a vision board does not have to be a tedious process. This can be a fun opportunity for a girls night, wine, and some creativity
Here is what you need to host your vision board party:
-Poster boards/Paper or Cork Board
-Magazines
-Scissors
-Glue
-Snacks
-Most Importantly Some Good Wine/Vino
Have a Method to Your Board
There is no right or wrong way to do this. I tend to divide my poster board into sections by category. Divide you vision board into 9 different sections. The top three sections of the board (from left to right) should be prosperity, reputation, partnerships/love. The second row should be family, health, and unity. The third row should be self-improvement, career, and travel. You can see a visual example of several options on Pinterest.
It is important to remember that you can change or update your vision board as much as you deem it necessary. I typically opt for the cork board version of the vision board because it is easier to modify. If you are hosting the vision board party and would like to utilize the cork board, it may be more cost-effective to collect those funds from your guests in advance, or request that they bring their own if they would like to use that.
Get Digital
Don’t have the time or resources to buy supplies for everyone? Get digital with your vision boards. There are several different ways that you can complete a vision board digitally by downloading simple apps from App Store from Apple or the Android Market. I particularly like the Success Vision Board Application by Jack Canfield, the creator for chicken soup for the soul. You can also create one online at www.dreamitaliave.com.
Remember the law of attraction! Hang your vision board somewhere you will see it daily. Use it to inspire you and generate positive energy at the beginning of your day. Live and work towards your dreams every day.
The beginning of a new year is a common time to reflect on the previous year, and deciding what goals you would like to accomplish in the next 365 days. This is not a time to be shy about the things that you want in your life. Be bold, intentional, and brave when setting goals for yourself. The sky is not the limit; it is simply the view. Although we tend to start out highly motivated and dedicated to the goals that we have set, we have got be honest with ourselves and realize that often that ambition can fade, and nothing gets accomplished! I want to share with you five methods I utilize to keep myself grounded, motivated, and a realizer of my goals.
Find Yourself a GOAL MATE
What is a GOAL MATE? A goal mate is someone that you have a great connection with that supports, motivates, encourages, and enables you to manifest all of your wildest dreams. It does not matter how far-fetched they may seem, your GOAL MATE will not only hold you accountable but encourage you to jump in and get dirty neck first. Whether you succeed or fail at accomplishing a goal they are there to pick you up if you break your neck for real (just kidding), brush you off, and send you on your awesomely merry way to attempt your next goal. Keep in mind, that in order to be a good GOAL MATE, you need to reciprocate the same energy and tenacity that your partner(s) give to you. It’s important to keep each other focused, interested, and motivated.
Make Clear, Objective, and Achievable Goals
Be clear and intentional about the goals you are setting. It is also important to be specific. Think about where you want to be with your finances, health, career, and love life. Self-love included. Be realistic with your timeline and remember that there are only 12 months in a year, but that is a valuable time that can be leveraged to generate a better you.
Make a Vision Board or Host a Vision Board Party
This is an annual tradition of mine. Each year I invite my GOAL MATES, friends, neighbors, co-workers over to craft vision boards. This is inexpensive and so much fun. All you need is magazines, scissors, glue, posters, your imaginations, and perhaps some wine!
Set Mall Quarterly Milestones
Hold yourself accountable. Think about where you want your progress to be after 3,6, and 9 months. I like to review my goals monthly. This keeps it relevant in my mind. You should review your goals quarterly at a minimum. Think about what is working for you, and what you can switch up.
Look at It
If you do not see your goals periodically, or place your vision board somewhere that you can see it every day. I have my goals on my vision board, iPhone, iPad, and posted in my locker at work. Don’t forget the plans you have made for yourself. Utilize these tools, go forth, and prosper!
Jazmin Nicole is a military officer, obstetrics nurse, advisory board member of Black Nurses Rock Inc., and the founder/CEO of Jazmin Nicole & Co.
www.iamjazminnicole.com
For more posts/blogs like this follow me on twitter (@jazminweb), Instagram (@therealjazminnicole_, and Facebook (Jazmin Nicole and Co.)
In an effort to combat the major health issues plaguing American Indians, the University of Kansas Medical Center and the American Indian Health Research and Education Alliance announced plans to create a Center for American Indian Community Health, with help from a $7.5 million grant from the National Center for Minority Health and Health Disparities and the National Institutes of Health. This new Center is sure to bring some much-needed care to the American Indian community, through improving education, outreach, research, and community resources.
Compared to the U.S. population as a whole, American Indians are astronomically disproportionately affected by a number of diseases: they are 420% more likely to die from diabetes, they are 100% more likely to die from tobacco-related illnesses, they have the lowest screening rates for breast and colorectal cancer, and they have the lowest five-year cancer survival rate.
Researchers plan to use the grant money in their efforts to recruit American Indian high school and college students into the health sciences programs at University of Kansas. No American Indians had been enrolled in the programs until recently. Now, three students have graduated, five are enrolled, and several more should be matriculating. Outreach has also been performed at the Haskell Indian Nations University to find students who might be interested in the public health program.
Historically, American Indians have been very distrustful of outsiders, including medical care providers, after a tumultuous and tragedy-filled history since explorers first came to America. The hope is that these graduates will return to their communities to improve the quality of care and work toward eliminating health disparities.
“Just being born American Indian brought me into the legacy of harm and poor health,” asserts Roxanne Struthers, RN, PhD, CTN, assistant professor at the University of Minnesota School of Nursing in Minneapolis and president-elect of the National Alaska Native American Indian Nurses Association (NANAINA). “I have seen in my family the effects of disease–TB and other epidemics with no resistance and little or no treatment. And not only disease [but also cultural loss]. My mother’s first language was Ojibwe; she was beaten when she spoke it, then her only language, at a rural reservation school. Later, she would not allow us to speak it at home. Now as a nurse, all the diseases I encounter every day [in Indian patients]–alcoholism, drug dependence, diabetes, overeating–I see as parallel to my own life. Some younger nurses may not be as aware of this at first, but it will resonate when they hear the history.”
“That’s when I started to see–and later I started to hear more,” recollects Lillian Rice, a Forest County Potawotami Tribe Native practitioner and alcohol/drug counselor, born in backwoods Star Lake, Wisc., and now living in Minneapolis. Then only 17 years old (in 1949), she linked the negative behavior of a close family member sinking into alcoholism with what she had heard earlier as a child from her grandmother. The grandmother had told of TB epidemics and children’s deaths, of scarlet fever quarantining with confiscation of Native ceremonial paraphernalia, of relocation without treatment or recompense, of going back home and finding the old estate burnt down by the U.S. government. Other family members brought forth painful memories from boarding school days of horsewhipping and humiliation.
“That’s when I decided to become a healer,” says Rice, who leads women’s sweat lodges and women’s spiritual gatherings. “After raising my five children and getting into chemical dependency work, I made a decision with a promise to the Great Spirit to be there for [Indian] women in honor of my grandmother.”
Lea Warrington, RN, BSN, gives a presentation on historical trauma to nursing students at the University of Wisconsin-Milwaukee.
“If you are Native and born into a Native family, your community’s past is a part of who you are,” attests John Lowe, RN, PhD, a faculty member at Florida Atlantic University’s College of Nursing in Boca Raton and a researcher/designer of Native American teen interventions to prevent and reverse substance abuse and reduce HIV/AIDS risk. “I was raised in a Cherokee farming community in the Southeast and went to school there,” he says. “My father, now 80, would have had to go to boarding school, so he didn’t go to any school. He was needed on the farm and his parents did not want their kids taken away. [I used to wonder,] why didn’t my father have the problems we see so often [in Indian communities], such as alcoholism and diabetes? Why was he OK? When I went away to attend a college nursing program in the 1970s, I took with me that vision of my father. He knew who he was: Cherokee, with traditions, values and beliefs. He faced many barriers, but something within him was very grounded and centered, and that kept him OK. If we [as nurses] could understand it, that is what we should promote.”
These Native American health practitioners are describing historical trauma. Although of recent coinage as a term, its devastating effects on the physical and mental health of American Indians and Alaska Natives have been documented for decades. Native healers, with their feeling for root causes, have tapped traditional spiritual resources to help put their families and communities back on a path to recovery. Now, working right in the mainstream of Western health science, leading Indian health professionals and researchers have given the concept a scientific name and a place for testing in their disciplines. The literature is now packed with empirical clinical evidence and qualitative data. Promising new models of care are emerging.
And today at the front lines, strategically positioned to put these models into practice, are Indian nurses. Their recognition of who they are and what they do has inspired a call to action for Native nurses: to recognize the critical role they can play in helping their people begin the process of healing from the harms of historical trauma.
Connecting, Listening, Empowering
John Lowe, RN, PhD
How does the healing start? For Native nurses, it begins with knowing yourself, your community and your common past.
“First, heal yourself,” urges Struthers. “The healing of one is the healing of all. Then you can share [with patients]. It does ripple out. You can reassure your patients by saying, ‘You are not unusual, you are not alone.’ History lessons are OK, too.”
Rachel Wright, RN, BSN, a master’s student in the nurse practitioner program at the University of Oklahoma College of Nursing in Oklahoma City, talks in terms of empowering patients.
“In fact, I think that’s the main thing nurses can do,” says Wright, whose father is Cherokee. “I agree that I see many Native American patients with social problems associated with physiological problems, but I believe that some of those are related to the self-esteem issue, lack of knowledge and lack of confidence to make lifestyle/behavioral changes that impact their health status. Any patient who feels like a failure and does not understand the problem most likely will not comply with the treatment plan. The nurse or nurse practitioner must help patients learn appropriate knowledge and skills to help themselves.”
To get compliance and accurate information from your patients, make sure the communication connection is two way, advises Lea Warrington, RN, BSN, manager of the Gerald L. Ignace Indian Health Center, an urban Indian Health Service facility in Milwaukee. Warrington, who is of Menominee Indian heritage and visits the reservation frequently, often finds out what’s really going on with her patients–as opposed to what’s in the clinic record–when she encounters them on their own “turf.”
Communication failure may come from passivity or not wanting to cause conflict, Warrington warns. Take the case of a 72-year-old patient whose daughter found all his medication bottles unopened in his medicine cabinet. The patient’s record at the clinic showed that he had very literally answered “yes” when asked whether he had filled his prescriptions and “no” as to whether he “had any problems with them.”
Often, after patients leave the facility, Warrington hears complaints about the way the clinic works, or about problems with service, that never showed up on the returned patient satisfaction surveys (usually checked off as “excellent”). “Outside the clinic, even though I work there, patients open up because we are in our own common setting, such as the elderly center, the school or on the street,” she explains.
Native nurses who work within the mainstream Western health care system face a paradoxical challenge, Warrington adds. “I believe that Native patients appreciate that Natives work in health care centers,” she says. “But I think, though, that sometimes we end up having to prove that we can provide as good service as non-Natives. It’s an odd situation to be in, because of the way Native people perceive the overall health care system as not being Native-friendly.”
Reducing Suicide Risks
“Start off with questions checking for traditionality and family connectedness,” suggests Dan Edwards, DSW, director of the University of Utah School of Social Work and Native American Studies in Salt Lake City. This information is essential for effective assessment, particularly in the mental health area, such as evaluating suicide risk.
Three first questions, suggests Edwards, might be: Where do you live? Do you know the [tribal] language? Have you ever been to your own tribal ceremonies? (For example, a female patient could be asked, “Have you ever been to a kinaalda [a Navajo coming-of-age ceremony for girls]?”) Then, he says, “as you establish rapport and if the patient seems open to it, you can begin talking about spirituality and religion.”
[ads:other]
Edwards is of Yurok heritage, with pre-1970s personal experience with foster care, adoption, boarding schools and assimilation pressures. He has observed the links for bad parenting and high divorce rates, heavy drinking patterns, vulnerability to negative peer pressures and suicide clusters.
Alaska Natives and American Indians rank first among all ethnic groups in suicide rates. While the particulars vary for subgroups–e.g., Indian people living in cities versus rural areas and reservations–the causes can be traced to historical trauma.
“The lost birds–Native Americans who were adopted out or in foster care and have completely lost their culture–are at high risk for suicide and/or risk-taking behavior if they have not successfully taken on their new family’s ways to a level of comfort that will offset these problems or if they have not sought their own culture later in life,” explains Margaret P. Moss, RN, DSN, assistant professor at the University of Minnesota School of Nursing and a Native Investigator (Hidatsa/Lakota background) in research.
Getting the complete family and lifestyle picture is also critical for suicide prevention in Indian teens and young adults, a particularly high-risk group, adds Faye Annette Gary, RN, EdD, the Medical Mutual of Ohio Professor of Nursing for Vulnerable and At-Risk Populations at Case Western Reserve University’s Frances Payne Bolton School of Nursing in Cleveland.
Gary, who gave a presentation on Native adolescent health and preventive education at NANAINA’s ninth annual Summit in Park City, Utah, last September, urges Native nurses to recognize the profile: male, between 15 and 24; single; likely to be under the influence of alcohol before suicide attempt; lived with a number of ineffective/inappropriate parental substitutes. Familiar historical trauma issues include “once a resident in boarding schools with frequent moves,” “in confinement centers at early age” and “experienced a loss of a significant other through violence.”
Healing Through Reconnecting
Defining Historical TraumaMaria Yellow Horse Brave Heart, MSSW, LCSW, PhD, research professor at the University of Denver Graduate School of Social Work, is the initiator and primary developer of historical trauma theory, intervention models and curricula. She defines historical trauma as “cumulative emotional and psychological wounding across generations, including the lifespan, which emanates from massive group trauma.”Brave Heart introduced historical trauma theory and applications in the late 1980s when she started to see her Lakota Indian community’s past as a linked sequence of “unresolved grief.” She defined the concept and developed grief resolution interventions to deal with specific phases in the historical trauma and responses to it. Her pioneering research has been disseminated in numerous publications and through workshops and community education she provides through The Takini Network, Inc., in Rapid City, S.D. ([email protected]).Brave Heart’s definition has been adapted by Native nurse researchers Roxanne Struthers and John Lowe in their work on nursing interventions for healing historical trauma in Native Americans.1-5
To get ideas for meeting the toughest health care challenges, such as diabetes, periodically review the Native American nursing literature–especially the articles published by Struthers, Lowe and other Native nurse researchers as part of the ongoing Nursing in Native American Culture project (see “References” and “The Conceptual Framework of Nursing in Native American Culture” sidebar).
Diabetes, suggests Struthers, can be looked at in a current community context along with a racial memory of the past–the taking of Indians’ land, with no more hunting and fishing; forced relocation interfering with diet and exercise; and the poor food choices that come with poverty.
Talking circles–community sharing groups based on Indian tradition–are being tried in many places to help patients deal with diabetes self-management and emotions. In two circles (for diabetes and domestic violence) at the urban clinic where Warrington works, patients learn to listen as well as talk, taking turns with “the talking stick.” The groups start by smoking cedar or sage in a shell (sometimes called smudging), which has a calming effect, and then close down the circle the same way.
Lowe offers a scenario, summarized below, showing how the conceptual nursing framework’s connectedness dimension might work for an Indian patient with diabetes:
► The nurse listens to a patient describe how he has been managing his diabetes. She is seated next to him about one foot away. There may be long periods of silence, but the nurse appears comfortable and does not ask demanding or threatening questions.
► Conversation ensues, centered around who the patient’s family members are and his everyday life and activities. The nurse talks about the community the patient lives in and resources available.
Solving the “Indian Problem” by Breaking the Tribal Bond: Federal Policy on Indian Health, 1850-1950Assimilation was forced through:Illness/murder (reservations; laws restricting free movement; food withheld or stockpiled and no hunting/fishing allowed; disease with no medical treatment; resistors sent to prison, murdered)Boarding schools (kidnapping; personal humiliation; renaming and little to no contact with families; abuse; survivor syndrome, failure to fit in, intergenerational family bond breakdown)Urbanization/relocation (promised jobs, housing and financial support did not materialize; those returning home no longer fit in)Termination/allotments (61 Indian tribes terminated in late 1950s to early 1960s; large tracts of land signed over without consent of the population; created internal war and conflict; damage from destroying land base of people who saw themselves as part of the land)Genealogy–Dawes Act of 1887 (identify Indian by blood quantum; can claim only one tribe; those less than ¼ of any tribe not “Indian”; disruption of Indian identity, family, clan ties)
► As the patient talks about the foods he eats, the nurse does not act condescending in her reply about foods he should be avoiding. Instead, she talks about alternatives and options available to the patient. The nurse knows that family and community must be involved and that the patient may need to be encouraged to use them as a resource and to allow them to help him.
► The nurse remains nonjudgmental by respecting what the patient shares. He is encouraged to talk and holistically express who he is in his everyday life and activities, his beliefs, his strengths, his management of his diabetes, and who he is connected to, such as family, community and other elements of the creation/universe. There may be storytelling and the nurse may share similar experiences.
► Native American nurses sometimes connect at a deep indigenous “oneness” level when caring for another Native American, especially in talking about how the past, present and future have affected them in similar ways.3
And finally, for a tested model of customizing interventions for a specific tribe, review Lowe’s ongoing work on Cherokee self-reliance and its application to substance abuse and other nursing interventions for teens.4 On a lifelong quest to understand what kept his own Cherokee father “OK” in the midst of cultural devastation, Lowe has analyzed the historical trauma dealt repeatedly to Cherokee men and the misguided policies and health concepts imposing non-Cherokee notions of independence.
Revealing the true Cherokee conception of self-reliance, which rests on being responsible, being disciplined and being confident, has produced a model that will work for holistic nursing assessment of Cherokee patients. Promotion of the core Cherokee value of interdependence promises to help overcome many of the ills that have come from disconnection and non-Native concepts of self.
References
1. Struthers, R. and Littlejohn, S. (1999). “The Essence of Native American Nursing.” Journal of Transcultural Nursing, Vol. 10, No. 2, pp. 131-35.
2. Lowe, J. and Struthers, R. (2001). “A Conceptual Framework of Nursing in Native American Culture.” Journal of Nursing Scholarship, Vol. 33, No. 3, pp. 279-83.
3. Lowe, J. (2002). “Balance and Harmony Through Connectedness: The Intentionality of Native American Nurses.” Holistic Nursing Practice, Vol. 16, No. 4, pp. 4-11.
4. Lowe, J. (2002). “Cherokee Self-Reliance.” Journal of Transcultural Nursing, Vol. 13, No. 4, pp. 287-95.
5. Struthers, R. and Lowe, J. (2003). “Nursing in the Native American Culture and Historical Trauma.” Issues in Mental Health Nursing, Vol. 24, No. 3, pp. 257-72.