The life expectancy of Californians decreased by about three years as a result of the COVID-19 pandemic, according to a study by UCLA researchers and colleagues published in the Journal of the American Medical Association.
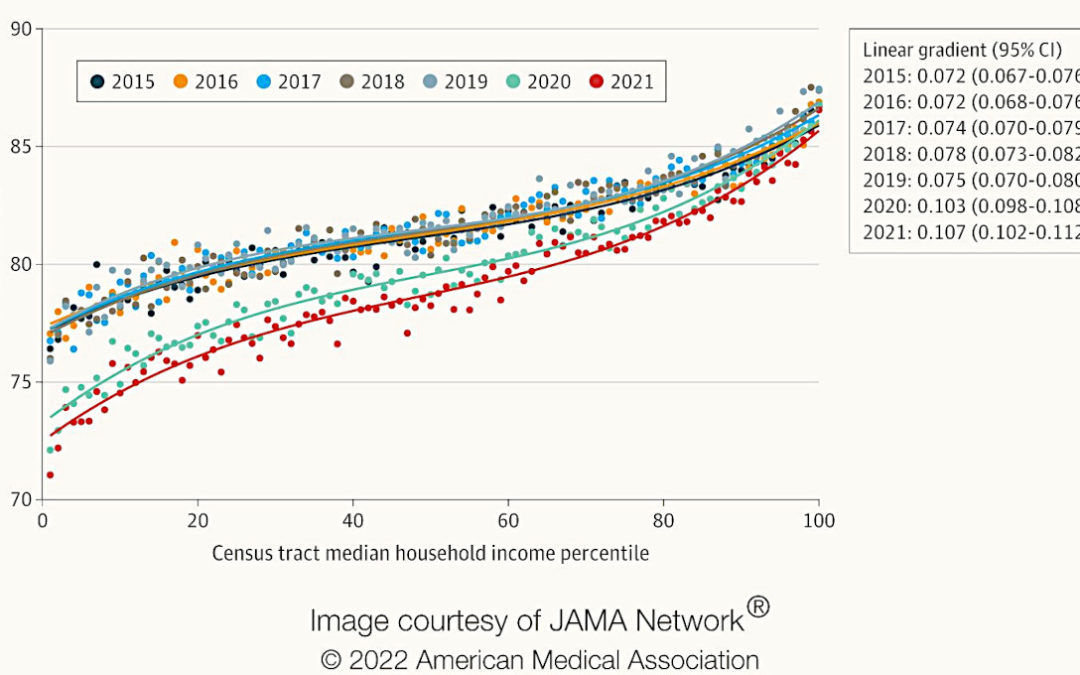
The research further shows that life expectancy for Hispanic, Asian and Black Californians decreased more than for white Californians and that the gap in life expectancy between those living in the highest- and lowest-income census tracts increased, from a difference of about 11.5 years before the pandemic to more than 15 years in 2021.
“Our findings are another troubling sign of how the pandemic’s impact was not felt evenly across all communities,” said study co-author Till von Wachter, a UCLA professor of economics and director of the California Policy Lab’s UCLA site. “Policymakers can use these findings to craft a more equitable response now, and also to inform how we plan for future public health crises.”
In their analysis of 1.9 million deaths in California between 2015 and 2021, the multi-campus research team calculated that life expectancy for Californians fell from 81.40 years in 2019 to 79.20 years in 2020, and down to 78.37 years in 2021. This study demonstrates that the reduction in life expectancy continued from 2020 into 2021, despite the availability of vaccines for much of 2021.
Life expectancy is not the average life span of individuals in a society but a hypothetical measure based solely on the mortality rates observed in a given year. It estimates how long a cohort of newborns could expect to live if it experienced the mortality rates of that specific year throughout their entire lifetimes. In the current study, life expectancy captures how much life was lost collectively within a population during the pandemic years, and it illustrates the dramatic differences in the pandemic’s impact across communities of different socioeconomic status.
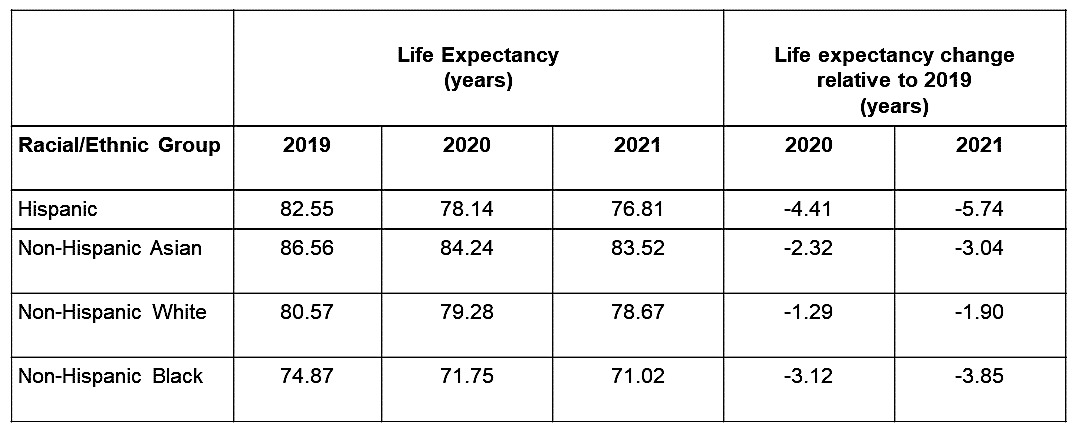
Hispanic populations in California lost 5.7 years of life expectancy between 2019 and 2021, while Black populations lost 3.8 years, Asian populations lost 3.0 years and white populations lost 1.9 years, according to the study. During this time, income also became more tightly correlated with life expectancy than it had been previously.
“We’ve had indications that the pandemic affected economically disadvantaged people more strongly, but we never really had numbers on actual life expectancy loss across the income spectrum,” said lead author Hannes Schwandt, an assistant professor at Northwestern University’s School of Education and Social Policy. “I am shocked by how big the differences were and the degree of inequality that they reflected.”
The study is based on an analysis of restricted death data obtained from the California Comprehensive Death Files maintained by the California Department of Health.
“In California, Hispanic individuals have historically lived longer than white individuals, but the pandemic upended that, as the life expectancy for Hispanic Californians decreased by about six years, three times as high as the decline for white Californians,” said co-author Jonathan Kowarski, a research fellow at the California Policy Lab and a doctoral student in economics at UCLA.
In addition to Schwandt, Von Wachter and Kowarski, study authors include Janet Currie of Princeton University, and Steve Woolf and Derek Chapman of Virginia Commonwealth University.
All my life I have rarely been sick, in fact there have only been two times that I can recall. So, about three months ago when I started feeling bad, it was out of the ordinary. I did not have any obvious symptoms, such as nausea, vomiting, headache, runny nose etc. I just had a lack of energy and no appetite. During this time it made me realize that “I would rather have great health, more than any material thing”; not that I do not like nice things or places. As children, many of us dreamed of growing up and having lots of money, big houses, cars and anything else that money could buy. We were only focused on the “material” things. There were never any thoughts about our physical or mental health.
I would rather have excellent health, than all of the money in the world. If you are sick and cannot get around, what good is having money and things, if you cannot enjoy it? Some people may say that they would use their money to hire the best doctors, but that is no guarantee that you will have good health. I often think of our patients that we are taking care of in the hospitals and clinics, they are relying on us to give them the best possible care to make them feel better. During this time, they become dependent on the healthcare staff and this may be hard for many that are used to having control of their own lives. Before you make an assumption that the patient is “difficult” or “hostile”, remember that these are people that were working, taking care of themselves and families and making their own decisions. We need to include them in all aspects of their care, instead of dictating what will be done. Although we may have our daily assignment planned, discuss with the patient the Plan of Care and let them have some input on the order of some things, to give them that feeling of control. We still have to stay on task, but we need to make them feel like adults and not like children being told what to do. Some people may think that this will interrupt your normal day, but imagine if it were you laying in that bed, how would you want to feel?
I have decided that I am going to enjoy life, spend more time taking care of myself and creating experiences with my daughter. I have been privileged to accomplish a lot of things in my life: writing my first children’s book, starting a home-based travel business, building my photography portfolio, traveling domestically and internationally; all while being a mom and nurse. We spend a lot of time taking care of others; but we must start taking care of ourselves; otherwise we will not be here for others.
So, the fatigue and loss of appetite that I was having was due to my Vitamin D level being critically low. I am currently working remotely, so eight hours of my day is spent inside on the computer. When I get off work, I wait until the sun goes down to go on my evening walk; therefore I was getting minimal to no sun. I am happy that this is a condition that can be easily corrected by diet, taking nutritional supplements and spending a few minutes sunbathing (in moderation). The benefits of sunlight is that Vitamin D is produced when your skin is exposed to the sun and it is one of the many vitamins our bodies need to stay healthy, relieve stress and increase energy.
I realized that work will be there; so I have made it a point to sit outside on my breaks and lunch. I am glad to say that I am feeling a lot better now. Never take your health for granted. You only have one life and you need to make sure to maintain your health. Take care of yourself, mind, body and spirit. The six best doctors in the world: sunlight, exercise, rest, diet, self-confidence and friends. Maintain them in all stages of life and enjoy a healthy life. Remember Health is Wealth!!
Nurse-midwives and educators from three prominent research universities have teamed up to improve pregnancy outcomes in Black communities by providing specialized training for doulas, persons who support birthing mothers and families through the entire process of childbirth.
The Alliance of Black Doulas for Black Mamas is led by Vanderbilt University School of Nursing Associate Professor Stephanie DeVane-Johnson, PhD, CNM, FACNM, Duke University School of Nursing Assistant Clinical Professor Jacquelyn McMillian-Bohler, PhD, CNM—both graduates of Vanderbilt’s nationally-recognized Nurse-Midwifery program—and University of North Carolina School of Medicine Assistant Professor Venus Standard, MSN, CNM, FACNM. The project leaders are Black, certified nurse-midwives with a combined 60+ years of midwifery experience.
Doulas offer emotional and informational support for pregnant persons and their families. Unlike nurse-midwives, they are not medically trained; however, their help with things like breastfeeding, acupressure, birth plans and postpartum issues can be critically needed, as can their presence as an advocate for the mother.
The three researchers are addressing the U.S.’s Black maternal health crisis. The U.S. has the highest maternal mortality rate among developed countries—and the crisis is even more pronounced for Black mothers. Centers for Disease Control and Prevention statistics reveal disparities between pregnancy complications and risks across different racial groups. Black women are approximately twice as likely to have a moderately low birthweight child and three times as likely to have a very low birthweight child than white or Hispanic women (https://www.cdc.gov/nchs/products/databriefs/db306.htm). Black women are also more likely than white or Hispanic women to die from pregnancy complications—almost 67 percent of which are preventable.
Having a trained and trusted professional who can help parents-to-be make healthy decisions and choose proper prenatal care can make a difference in maternal health and birth outcomes.
DeVane-Johnson, McMillian-Bohler and Standard worked together to write and fine-tune a plan to train and provide Black doulas to help Black families, with hopes of mitigating the high Black maternal and infant mortality rate. In 2020, the doula project was funded by a $75,000 award from UNC, the Harvey C. Felix Award to Advance Institutional Priorities and the group trained its first 20 doulas. In 2021, they received a $545,000 Duke Endowment grant, which will fund the program for three years beginning in May 2022.
Nurse-midwives Jacquelyn McMillian-Bohler, Venus Standard and Stephanie DeVane-Johnson.
The main program goals are to: decrease Black maternal mortality and morbidity; improve patient experiences; provide doulas for free to families; and help those interested in becoming doulas build critical skills and later use those skills to earn wages. The program’s goals align with the 2021 Black Maternal Health Momnibus Act, which “directs multi-agency efforts to improve maternal health, particularly among racial and ethnic minority groups, veterans, and other vulnerable populations,” states congress.gov (https://www.congress.gov/bill/117th-congress/house-bill/959).
“The training is more than about labor and birth,” said McMillian-Bohler, who teaches the mindfulness curriculum. “We also introduce the doula to general stress-reduction techniques such as mindfulness and acupressure. Although evidence suggests these techniques are helpful, they are often not accessible to the Black community.”
DeVane-Johnson works remotely as the community engagement liaison for the program, which is housed at UNC Family Medicine in Chapel Hill, but the doulas will be serving families in Durham, Wake and Orange counties in North Carolina. Devane-Johnson hopes to receive funding to expand this program to Black pregnant persons in Nashville, TN.
“The strength of the program is the expertise of the entire team and the integration of the expertise,” said Standard, who connects families with doulas from the program and is currently teaching the third cohort of Black doulas. “Although each university could independently support the doula program with its hospital system and academic affiliation, a collaboration between the three universities positively impacts the project as a whole.”
Doula training applicants attend information sessions and are screened to make sure they will be successful in the program and that they will enjoy the work.
According to McMillian-Bohler, the program’s doula/family partnerships offer racial concordance, which can increase trust and understanding.
“I think the fact that we are able to come in and talk about some of these health resources and, I hope, remove some of the stigma, opens up a whole area of health care and wellness to people who desperately need it, who maybe didn’t feel like it was for them,” McMillian-Bohler said.
The doulas recognize that birthing parents have the right and need to speak up for their own bodies and health, and help them build the confidence and ability to do so.
To receive help from a doula in the program, a person must be Black, pregnant and planning to deliver at a University of North Carolina-affiliated hospital.
“By having a culturally concordant doula, the patient has a personal advocate, educator and support person to help guide and navigate the system as a Black person, whose needs are often dismissed or ignored,” Standard explained.
“Our hope is that by selecting doulas, who are gatekeepers into various aspects of the Black community, and by giving them tools to share with families, we create a community project that helps birthing families and doulas, said McMillian-Bohler”
The program offers doula training that is expanded to accommodate the specific needs of Black women, covering topics like reproductive justice and the “superwoman schema,” which says that many Black women care for others at their own expense, increasing stress during a pregnancy.
“The goal is to help mitigate Black maternal and infant mortality rates,” DeVane-Johnson said. “Doulas stand in the gap. Sometimes, Black women bring things up to their health care providers and are not taken seriously, or the provider does not talk at a level that the patient and family can understand. The doula is there to bridge that gap and potentially interpret information.”
DeVane-Johnson also serves as the facilitator for breastfeeding lectures. She studies the history of breastfeeding and presents lectures to doula-trainees to help them understand the hurdles faced by those they are trained to help. The doulas use this training to support Black women who want to breastfeed and connect them with lactation consultants, as research indicates that breastfeeding decreases cancer risks in mothers and improves health outcomes for babies.
“Black women have the lowest breastfeeding rate out of any race,” DeVane-Johnson said. “When variables such as socioeconomic status, education and marital status are controlled for, similar positioned white women still tend to breastfeed at higher rates.”
Doulas help solve communication issues and offer consistent labor support for those who don’t have it, something that has been shown to decrease time in labor and the need for pain medications.
“We hope to create opportunities for Black women to find their voices and be empowered to ask questions,” McMillian-Bohler said.
“Doulas are there to empower, uplift and elevate birthing families,” she continued. “If something doesn’t feel right, the doulas help them recognize that they need to speak up and keep speaking until their voice is heard.”
The doulas are trained to recognize preterm, term and postpartum warning signs that may otherwise go untreated, leaving parent and baby at risk.
They train over the course of seven weekends. While on-call with patients, they assist with birthing plans, help pack bags for the hospital and even attend appointments, depending on how much support the birthing parent needs. Once trained, a doula is paired with three Black families who receive assistance for free.
DeVane-Johnson says program applicants need to be Black, have a passion for birth work and have a desire to support women in labor. In the past, applicants may not have been financially able to secure training, but thanks to the grants, training is free.
Applicants are screened to make sure they have reliable transportation, a job that’s flexible enough to allow them to leave to attend a birth and are vaccinated against COVID-19.
According to DeVane-Johnson, the most important qualification is “a passion to help support Black families in the community.”
“Being a doula often is different than what many people imagine,” said McMillian-Bohler. “They may have a romanticized notion of what the job is like. Babies come all the time, anytime, and doulas have to be able and willing to drop whatever other things they may be doing to come to a birth.”
The program benefits go beyond those received by the birthing family.
“Doulas are marketable and can hire out their services after they work with their first three families through the program,” DeVane-Johnson said. “This training will help them bring in money for their families and provide an important service.”
The program supports workforce development, DeVane-Johnson said, as the new doulas have sustainable jobs and develop entrepreneurial skills.
With many interested in training and families lining up for the service, the program is poised to make a difference in communities and in Black maternal health—and the leadership team envisions it as something that can go even further.
“Our goal with this program is to create a doula training model that can be tailored for birthing people with disabilities, those in the LGBTQ+ community, making things culturally relevant to whatever specific marginalized population that is birthing, because it’s these marginalized populations that have the worst birth outcomes,” DeVane-Johnson said.
At this time, the program has one year of data and the group looks forward to evaluating the incoming qualitative and quantitative data, something the new Duke Endowment grant will help them do over the course of the next three years.
DeVane-Johnson, McMillian-Bohler and Standard also hope to see the program expand beyond the borders of North Carolina.
“We want to disseminate this program throughout the country,” Standard said. “We want to reach out to other academic hospital-affiliated institutions and integrate this program into their maternal care systems.”
If the program receives additional funding, Standard said they plan to increase compensation to the doulas and faculty, and hire additional staff to support an expansion to help more families.
In January 2009, the Maricopa Integrated Health System (MIHS) staged the grand opening of the Refugee Women’s Health Clinic in Phoenix, Arizona with Dr. Crista Johnson, MD, FACOG as the founding medical director. It is believed to be the only such clinic in the U.S. specializing in obstetrics and gynecology for refugee women from Africa, Asia and the Middle East.
“What was striking,” said Dr. Johnson, “was the language, the cultural barriers and the stress the women experienced when they would come to the hospital. The clinic will be an oasis to the community because there will be trained staff, knowledgeable regarding care services, resources, and specialized information who understand the patients better, and are able to facilitate a positive patient experience during their hospital contact and even in their homes.”
“These people,” Dr. Johnson continued, “are called navigators and they include nurses, public health workers, lay workers and others who would serve as a resource guiding, interpreting, communicating, facilitating and helping the refugees through the often times complicated and unfamiliar processes in obtaining satisfactory health care services.”
In the case of the refugee, who most know very little about seeing a doctor, or receiving clinical treatment, or home care of any sort and are also totally lacking in exposure to allied health services. But the engagement of navigators to improve certain service outcomes, and ultimately access to services, added a dimension that has made the service provider a key contributor to the improvement of patient satisfaction.
Duke Health in 2011 launched a robust and credible initiative using a class of employees as navigators who would serve as a resource to patients who because of cultural, economic, historical life experiences, or other reasons needed assistance in facilitating their engagement with the healthcare provider.
“The mission of the intervention,” said Dr. Angelo Moore, PhD, Assistant Director and Program Manager for Community Outreach, Engagement, and Equity (COEE) with Duke Cancer Institute, “was to be part of a highly visible community overall strategy to achieve care delivery that was equitable, culturally appropriate, and timely. The desired result would contribute to improved community health, higher performance outcomes and patient satisfaction.” The mechanism that would be employed is referred to as patient navigation. This is a concept and a process first introduced in 1990 by Dr. Harold Freeman a surgeon who saw the need for a resource for his cancer patients in Harlem Hospital, New York and who were predominantly African American women.
Dr. Freeman, who now oversees the operations of the Harold P. Freeman Patient Navigation Institute in New York, describes navigation as an individual intervention to help overcome barriers due to systemic reasons. “Patient navigation is what a person does,” says Dr. Freeman. However, the type of patient navigation that is employed is based on the education, skill set, scope and who is being served. In the market-place, and since the launching of the concept, several different titles have emerged such as Nurse Navigator, Resource Navigator, Community-Facing Navigator, Clinical Navigator, Non-Clinical Navigator, Lay Navigator. There is now an ongoing effort to harmonize these titles around a common set of descriptors common to the role and purpose of navigation.
Foundational to the role and purpose of navigation is the elimination of barriers or impediments.
What types of impediments are these? Examples of some of the frequently encountered barriers that may be eliminated through patient navigation: Financial barriers (including uninsured and under insured); communication barriers (such as lack of understanding, language and/or cultural competency), medical system barriers (fragmented medical system, missed appointments, lost results); psychological barriers (such as fear and distrust); other barriers (such as transportation and need for childcare).
Dr Freeman’s interest and desire to tackle the high percentage of African American women who were referred to him for diagnosis and treatment, was peaked when he saw that they were in the third and fourth stages of the disease of cancer. He took note that these women were also poor economically and lived very marginal lives, the circumstances that would impact their access to care. Dr. Freeman knew from available data that white women had a lower cancer morbidity rate. He decided to conduct an investigative approach to identify, if possible, the root causes of this phenomenon.
One of the core derivatives of his work was the description assigned to the title “patient navigator.” A patient navigator is a healthcare professional who proactively guides patients through the healthcare process. They are responsible for ensuring that the healthcare provider’s system met the needs of the patient as best as possible. To that end, patient navigators spend their time communicating with patients and their families and as an interface between the patient and the provider. They engage patients by describing the relevant options, the true nature of their illness, what to expect during the treatment process, and what their recovery process will be like. They may also need to identify what are the patient’s legal rights.
It’s important that patient navigators once able to convey the specific impediments that stand in the way of effective treatment, go in pursuit of remedies to overcome the obstacles that they may encounter while pursuing treatment. This means that employees in this role need to be highly knowledgeable of healthcare systems and what can be done to ensure the patient is provided the best possible care. Attributes of compassion, positiveness, trust-building and coaching skills are key to success as a navigator.
To do well in this role, it’s critical that the employee be able to answer patients’ questions as they arise. This means that navigators must have a strong understanding of healthcare systems and how they function. They should also be a compassionate, positive individual who is capable of inspiring confidence in the patients served.
Ultimately the impact of the work of patient navigation is embedded in the social determinants of care. This addresses the social, cultural, environmental, and economic conditions in society that impact upon health. In this regard, colleagues compile and disseminate evidence on what works to address these determinants, build capacities and advocate for accelerated action.
Changes in the status of women’s reproductive health and protections have been at the forefront of new headlines in recent weeks. The leaked Supreme Court documents indicating that the justices are on the precipice of turning over 50 years worth of reproductive health precedent has a lot of people pausing to consider the implications of losing something they have largely taken for granted. Many women are recognizing that if Roe v. Wade is overturned, they will have less bodily autonomy than corpses often have in their home states.
Of course, for many women – particularly minority women in deeply conservative states – these rights were slipping away long before this. In many of these states, the number of reproductive health clinics is extremely limited and causes undue burdens on women trying to access them. Multiple studies on the topic have shown that minority women, especially those from poorer backgrounds, are the most likely to face difficulties accessing any sort of reproductive healthcare than their more affluent, white peers.
Regardless of where our personal beliefs related to abortion rights fall, we can all agree that women having better access to reproductive healthcare is a valuable endeavor. For many nurses out there, this means striving to break down barriers that limit healthcare access. It also means becoming an advocate for health equity. But how does one become an advocate within their own community?
Address Inequalities
Many of the inequalities that nurses see every day aren’t easy ones to just address and deal with. Rather, they are ingrained, pervasive community and cultural issues that will take years to fully unpack and start to address in a positive manner. However, there are things that nurses can do to help address some of the healthcare inequalities that minority women face regularly.
Perhaps one of the most powerful things nurses can do to help address health disparities is to recognize and empathize with the differences. Minority nurses with a background in minority communities are in the position to play a unique and powerful role here. Who better to build a bridge of understanding and trust than someone who already has an understanding of the social, cultural, and economic factors that may be influencing healthcare choices.
Immediately addressing any form of blatant discrimination.
Advocating for policies that promote human rights and equity.
Working with numerous professionals across disciplines to ensure patients are receiving holistic healthcare.
Encouraging medical trials that are inclusive and address the concerns of minorities.
Seeking out and promoting other professionals that are striving to address equity issues in their communities.
Encourage Screenings
When working directly with patients there are a few things that can be done to help decrease health disparities. Arguably the most important is building trust in the community, which most certainly will not happen overnight. Small steps to start can include things like doing preventative health education out in the community, finding strategies that can help with payment for medical services, and being available for health-related questions without requiring an appointment.
Unfortunately, minority women are typically at greater risk for developing a number of diseases. For instance, African American women are twice as likely to develop breast cancer. Likewise, African American women are more likely to develop high blood pressure earlier in life than white women. There are many factors that influence this, but ultimately detection is one of the best forms of prevention.
Women can benefit from regular health screenings, but many are reluctant to do so. Going to the doctor’s office is uncomfortable, time-consuming, and potentially expensive. Helping women, especially minority women, understand the value of preventative health screenings over the long term is a vital role that nurses can play. Promoting more screenings can be one straightforward way to catch and treat issues before they become life-altering health problems.
Soft Skills Matter
Minority women, particularly women of color, are more likely to face negative health outcomes than other groups. Ingrained inequalities and cultural perceptions of the healthcare system play a major role in this. As nurses work to address these health disparities it becomes apparent that not only is a deep knowledge of nursing and healthcare important, but so are the soft skills that help convey the message.
For example, soft skills such as empathy are critical to understanding and adequately responding to the difficulties that some patients are facing. Empathy can lead to better, more realistic health prescriptions and outcomes. Patients are also more inclined to trust and listen to someone that shows an understanding and compassion for the information they are providing about themselves and their health.
Communication is another important factor. Even the best messages can be lost if they are not delivered in an understandable and relatable way. Patients do not like to feel talked down to and many very deeply want to understand the healthcare system before they have to make major decisions within it. Clear communication about procedures, health factors, costs, and outcomes are also imperative for building trust and making patients feel comfortable about their health choices.
Healthcare inequalities are significant for some demographics of the population, particularly minority women seeking reproductive healthcare. Nurses can make a real difference in starting to address some of these disparities by becoming advocates for their patients. It involves building trust, showing empathy, and encouraging positive health choices. None of it is easy, but it can add up to make a powerful difference in local communities.
In early December 2021, I was seeing a physical therapist for a shoulder injury. During one of my visits, the therapist was alternating between me and another patient on an adjacent bed, who had a knee replacement. While the therapist worked on the other patient’s leg, stretching it and bending the knee, I eavesdropped on their conversation.
The patient was in pain, anxious to complete the hard part of the therapy. The therapist was encouraging him to keep working. At one point the patient expressed a desire to quit. The therapist responded “Te queda una semanita más.” This translates to “You have a short week left.” The patient agreed to continue.
By adding the suffix “ita” to the word “semana,” – or week – the therapist offered the patient a perspective on how much therapy remained in a way that sounded shorter, even though it was still a full week.
This ability to minimize or exaggerate a situation by simply adding a suffix is one feature of the Spanish language that could contribute to a striking resilience in health that researchers have documented in Hispanic populations in the United States, called the “Hispanic Paradox.”
As a Hispanic quantitative psychologist, I have been involved in research on stress and cardiovascular health at the University of Miami since 1988. More recently, I joined the Hispanic Community Health Study/Study of Latinos as an investigator. This observational study of over 16,000 adults documents the health of Hispanics of various backgrounds in four urban communities in the U.S.
Heart disease killed 696,962 persons in the U.S. last year. The causes involve interactions between genetics and environmental factors such as smoking, leading a sedentary lifestyle and consuming a high fat diet. These behaviors contribute to heart disease and stroke.
Stress also contributes to heart disease. How people react to that stress is important, too. The extent to which our language facilitates how we process our emotions in response to stress may therefore be important in heart disease. For that reason, the Spanish language may offer an advantage. Having lived a bilingual life, I believe this to be true.
This seeming paradox between Hispanics’ higher health risk yet lower overall rate of heart disease came to be called the Hispanic Paradox. Prior to the COVID-19 pandemic, Hispanics lived on average three years longer than their white counterparts, according to the Centers for Disease Control and Prevention.
Family ties alone can’t explain the Hispanic Paradox
I became intrigued by this phenomenon when I joined the Hispanic Community Health Study in 2008. My first attempt at finding an explanation for the Hispanic Paradox led me to investigate whether the family unit might offer some protection against early life stress.
In that work, I estimated the prevalence of adverse childhood experiences in Hispanics in the U.S. If the family was a source of resilience, I expected to find low rates of experiences of abuse, neglect or family dysfunction. But to my surprise, the prevalence of these adverse events was actually quite high in those populations. In fact, 77% of the target population reported experiencing at least one adverse childhood event, and about 29% reported experiencing four or more before the age of 18.
That led me to the realization that the source of the resilience seen in the Hispanic Paradox did not necessarily come from the safety net of family.
Exploring how culture could contribute
I next turned my attention to other cultural resources such as social support and optimism, factors that may buffer the impact of stress.
Is the Hispanic culture more optimistic than the American culture? Having an optimistic view can help people think about stress as being temporary and manageable. Optimism can make a person feel they can cope with stress.
I came across a paper on the positivity of human language. The researchers had developed a “happy index” that they applied to measure the number of positive words in a variety of sources from several different languages. They analyzed books, newspapers, music lyrics and tweets, for instance.
A figure in the paper showed the distribution of the happy index across sources and languages. The result was startling. The sources with the highest happy index ratings were those in Spanish!
Once I identified the Spanish language as a focus, the pieces began falling into place. I relied on linguistic analyses to examine the role of language in emotion. A current theory of emotion describes how people need language in order for their brains to construct emotions. Research shows that emotions influence how blood pressure and heart rate react to and recover from stress. And our reactions and recovery from stress play a central role in the development of heart disease.
In other words, the rich and positive emotion lexicon of the Spanish language may not only influence culture over time, but also influence our emotional reaction to stress.
The contribution of verbs
However, it may not only be the positive words that are contributing to better cardiovascular health in Hispanic populations. There are other features of the language that facilitate emotional expression.
Take, for example, the two forms of the verb “to be.” In English, we simply “are.” But in Spanish, we can be a certain way temporarily – “estar” – or more permanently, “ser.” This comes in handy when considering negative situations. In English I could be overweight. In Spanish I can be permanently overweight, which translates to “ser gorda,” or I could be temporarily overweight, or “estar gorda.” The latter is transient and entertains the possibility of change, which can itself encourage motivation towards change.
Spanish is one romance language that makes use of the subjunctive form of verbs. The subjunctive expresses hypothetical situations, wishes and possibilities. For instance, consider the “magical realism” of the Colombian author Gabriel García Márquez. His use of the subjunctive facilitated the possibility of alternative realities.
The Spanish language’s ability to minimize and exaggerate by the simple addition of a suffix also increases the range of emotions and perceptions. This is how the therapist in the example helped his patient persevere through a difficult phase of therapy.
While English is the language of science – precise and succinct – my hunch is that the flowery nature of Spanish contributes to a culture that supports emotional expression. In doing so, it can help its speakers manage the responses to stress.