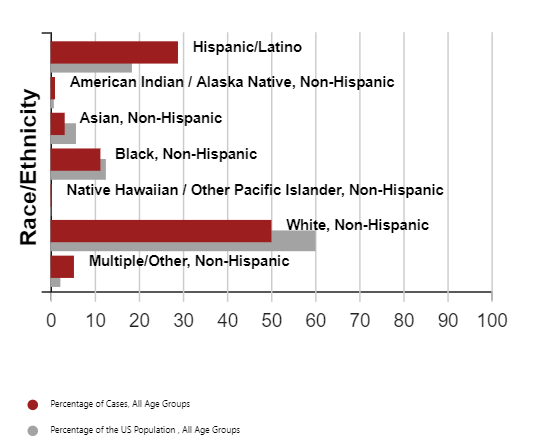
The coronavirus has hit minority communities harder in terms of health by amplifying social and economic factors while also revealing deep-rooted inequities. Racial disparities that were present before the pandemic have only been compounded and are evident in the rates of minorities contracting the virus compared with their percentage of the population. This has especially been seen in Latino and multiracial communities in the United States. According to the CDC, Latinos make up 18% of the population and account for nearly 29% of Covid-19 cases. Similarly, those who identify as multiracial (non-Hispanic) make up 2% of the population but 5% of Covid-19 cases.
Source: CDC Covid Data Tracker (as of 5/20/21)
As a result of the pandemic, racial and ethnic disparities in access to behavior health care have also been illuminated. Interestingly, the rates of behavioral health disorders in Blacks and Latinos do not differ from the general population. Yet, they do have markedly less access to mental health and substance-use treatment services. According to the Substance Abuse and Mental Health Services Administration (SAMHSA), of the 4.8 million African Americans that live with mental health disorders 69.4% of them receive no treatment. Of the 6.9 million Hispanics who live with mental health disorders 67.1% receive no treatment. Both these statistics are alarmingly high when compared with the 56.7% of the overall U.S. population that do not receive treatment for mental illness. Likewise, alarming numbers can be seen in those with substance use disorder. Of the 2.3 million African Americans who have Substance Use Disorder, 88.7% do not receive treatment. Of the 3.3 million Hispanics who have Substance Use Disorder, 89.7% do not receive treatment.
There are already many barriers in place for Blacks and Latinos due to social determinants that only increase the vulnerability of those with mental illness. Black and Latinos have lower access to health care, are found to terminate care prematurely, and receive less culturally responsive care. The opioid pandemic is perhaps hitting the Black and Latinos the hardest due to their limited access to preventive treatment and recovery resources for substance use disorders. Despite Blacks having comparable rates of opioid misuse as the general U.S. population, they were found to have the greatest rate of overdose methadone synthetic opioid deaths.
Nurses must work with the health care team to prevent the interruption of substance use treatment and recovery services. Telehealth services must be expanded. Those with substance use disorders and mental illness who have Covid-19 particularly need support during this time. Recovery support groups that have been stopped, clinics that have closed, and the discontinuing of harm reduction services like syringe service programs have the potential to trigger relapses in our patients as well as increase the rates of HIV and hepatitis. According to SAMHSA, Blacks and Latinos who have substance use disorders and mental health disorders are found to be more likely to be homeless and incarcerated which further increases their risk of Covid-19.
There is much potential for managing this identified risk and problem in Black and Latino populations. Policy efforts can be made in the form of disaggregating data so that resources can be targeted based on more specific data. Policies and treatments should be more flexible. For example, SAMHSA released a guide which enabled dispensable take-home methadone treatment programs during the pandemic. There should also be a push for expanded and flexible coverage of telehealth so patients can continue to receive treatment via the telephone or video-conferencing.
Communication, health literacy, and public awareness must also be accounted for. Covid-19 education should be translated into the language of those in the communities we serve. Also, messages should be culturally tailored so that concepts presented like social distancing are culturally appropriate. Communication channels are also important so perhaps using Black and Latino radio stations, websites, and trusted media figures to deliver important messages about prevention strategies
Workforce efforts can also be had by augmenting the workforce with culturally competent healthcare professionals. The workforce is in dire need of the individuals. Perhaps fast-tracking immigrants, refugees, and bilingual health care professionals could create a much needed pool of such health care workers in the United States. Peer navigators and coaches are also valuable for creating outreach and engagement of Black and Latino communities so that they can be properly linked with mental and substance use disorder treatment. Peer navigators know the communities we serve well and know how to effectively communicate with clients. These could be made virtual to ensure Black and Latino communities receive proper behavioral health care.
Blacks’ and Latinos’ physical health have greatly been impacted by the pandemic with a disproportionate rate of Covid-19 infection. However, the pandemic is not only affecting the nation physically—but also behaviorally. As nurses we address the physical and emotional health of our clients because we see them as a whole being. Therefore, we must work hard to address these issues and advocate for our patients so that they can live healthy lives, not just in their bodies—but in their minds as well.
Last December, the FDA reported on both the Pfizer-BioNTech and Moderna Covid-19 vaccine and the respective race and ethnicity of their research participants in the Phases 2 and 3 research trials. The Pfizer trial included ages 16 or older and the Moderna trial included those 18 and older. Of 285 million in the United States population, over 40 thousand participated in the Pfizer trials and over 27 thousand in the Moderna trial. When looking at the combined totals of subjects compared to the general population, whites were found to be over represented. Whereas 73.6% of the U.S. population are white, 79.4% to 81.9% of the subjects reported their race as white. American Indian/Alaska Native and Native Hawaiian or Other Pacific Islanders had the exact percentage of research participants to those of the U.S. population; 0.8% and 0.2%, respectively. The second largest contrast in proportion of participants to the U.S. population was seen in comparing those of Asian race. Only 9.7-9.8% of research subjects reported themselves as Asian, whereas the total U.S. population percentage is 5.9%. The biggest discrepancy can be seen in research participants who reported their race as Black. Only 9.7-9.8% of research subjects were Black, whereas Blacks make up 12.3% the current total U.S. population. Regarding ethnicity, 17.6% of the U.S. population reports themselves as being Hispanic and 20-26% of participants identified themselves of Hispanic ethnicity. However, 82.4% of Americans report themselves as non-Hispanic and 73.2% to 79.1% of research subjects identified themselves as that ethnicity.
Despite these Covid-19 vaccine trials demonstrating greater diversity than previous trials of other pharmaceuticals, these statistics still represent a disparity in the representation of people of color as research participants in a vaccine designed to boost the immunity of a virus that is disproportionately affecting people of color in the United States.
The good news is that despite this disparity in the diversity of representation in the clinical trials, the findings did show that the safety and efficiency of the Pfizer-BioNTech and Moderna vaccines were similar across groups despite race. The question many pose in reaction to such statistics is why minorities are underrepresented in clinical trials. The main four reasons include: barriers to access, lack of information, and historical and continuous racism and discrimination. Barriers to access come in the form of few clinical trials being offered through under-resourced hospital systems that minorities use for health care. Also, minorities are less likely to have eligibility to participate in such trials due to having co-morbid conditions or not having health insurance. These attributes can exclude them from participation in such research studies.
Other challenges to access may be their limited or lack of transportation resources, being unable to request off of work, caregiving schedules, or not having access to technologies for monitoring during a research study. Some research studies have reported that physicians are less likely to offer clinical trial participation to minority patients. Enrollment efforts of research studies often may not reach the minority population if they are not culturally sensitive to address language or health literacy barriers. The history of medicine in the United States also has seen the abuse and mistreatment of minorities such as the Tuskegee syphilis experiment. As a result of such abuse and ongoing racism and discrimination, minorities are less willing to participate in clinical trials.
The racial and ethnic diversity of clinical trials in the further development of Covid-19 vaccines is imperative. This pandemic has impacted those of Black adults and minorities the most, so more trials should effectively recruit and maintain the participation of minorities. Minorities already historically have had lower vaccination rates and express more concerns about receiving the Covid-19 vaccine and perhaps their concerns are valid based on the data presented in this essay. Therefore, it is important that Covid-19 vaccine researchers ensure the safety and efficiency of the vaccine across all of the United States to increase the trust and confidence of minorities that they should get the vaccine.
On April 3, 2020, the Centers for Disease Control (CDC) made a statement encouraging all Americans to wear cloth face coverings upon leaving their homes. In response, Black men have expressed their concern about such a recommendation. Their concern is based in that wearing masks could expose them to racial profiling and harassment from law enforcement officers. An example of such concern can be seen in the Twitter posting of Aaron Thomas, a Black man living in Ohio: “I don’t feel safe wearing a handkerchief or something else that isn’t CLEARLY a protective mask covering my face to the store because I am a Black man living in this world. I want to stay alive but I also want to stay alive.” Such a tweet has been reposted more than 18,000 times since its original posting. Based on his statement, Thomas has decided to not wear a mask so that he can “stay alive.”
This concern has not been unwarranted. A month before the CDC provided its recommendation, two Black men posted a video of themselves on YouTube being escorted out of a Walmart in Wood River, Illinois by a police officer for allegedly “wearing surgical masks.” One of the men stated that: “[The policeman] followed us from outside, told us that we cannot wear masks. This police officer just put us out for wearing masks and trying to stay safe.” The chief of the Wood River police, Brad Wells, stated later in a news release that the police officer in the video “incorrectly” told such men that a city law prohibited the wearing of masks. Chief Wells went on to state: “This statement was incorrect and should not have been made. The city does not have such an ordinance prohibiting the wearing of a mask. In fact, I support the wearing of nonsurgical mask or face covering when in public during the COVID-19 pandemic period.” As a result of the two men filling a complaint, Chief Wells told The Washington Post that an internal investigation of the incident has begun with the assistance of the local NAACP branch.
Georgia Senator, Nikema Williams, wrote a letter to the state’s governor urging him to temporarily suspend the mask laws. She explains why in her letter, stating that her husband, who is African American, 6’3”, and weighs 300 pounds: “was telling [her] how uncomfortable it was to wear a mask in stores because folks get intimidated and look at him like he’s up to no good.”
Black men have also experienced racial profiling when not wearing a mask. In April of 2020, a video from Philadelphia filmed a Black man being removed with force by four police officers one day after the city’s transportation authority required all riders of buses, trolleys, and trains to wear face coverings. After the incident, the transportation authority made an announcement deeming face coverings no longer required for riders.
Therefore, it has been found that both Black men who follow and do not follow the CDC recommendation to wear a face covering have experienced episodes of harassment. Blacks are already at an increased risk of contracting the virus, but now Black men in particular are faced with the dilemma to wear a mask to save their lives from either racial profiling or the raging COVID-19 pandemic.
Like several senators, the NAACP has also made a statement urging states to indefinitely stop their mask laws. Marc Banks, the NAACP’s national press secretary, stated: “No person should be fearful of engaging in lifesaving measures due to racialism.”
Melanye Price is a political science professor at Texas’ Prairie View A&M University. She tells The New York Times that the well-intentioned recommendation to wear masks or bandanas actually can put African Americans at greater risk of racial profiling. According to Kevin Gaines, a professor of civil rights and social justice at the University of Virginia, Black men are already being profiled by the police on a regular basis, but wearing masks heightens such risks of profiling. The initial assumption is not made that Black men are wearing masks to protect themselves and those around them from the threat of the virus. However, in contrast, it is assumed that they are engaging in some type of ill will like stealing or other crimes.
As a result of the risks of racial profiling, some Black men have changed their style of dress in an effort to appear less threatening. STAT correspondent Usha Lee McFarling reports that Black men have attempted to “tone down their appearance to lower suspicion.” Examples of such “toning down” comes in the form of wearing college T-shirts and “dressing like prospects, not suspects.” This has even been found in their choice of mask colors and patterns, choosing floral prints or plain white masks over others.
Vickie Mays, a professor of heath policy and management at UCLA, has been attempting to track situations in which Black men wearing masks have suffered harassment. Mays tells STAT that Black men should wear masks despite the risk of racial profiling in order to, foremost, protect their health. However, she suggests that such masks not be dark in color or “ominous looking.” Instead, she suggests they be bright in color or have traditional African prints. Mays also urges health officials to swiftly procure professionally-made masks for Black communities just as they would any other commodity like food or water as this population has been reportedly experiencing greater rates of COVID-19 infection than non-minority groups.
COVID-19 is hitting minorities harder than other communities. According to the Centers for Disease Control, as of June 12, 2020, the age-adjusted hospitalization rates were reported highest among non-Hispanic American Indian or Alaska Native and non-Hispanic black persons, followed by Hispanic or Latino persons. The CDC clearly states that such racial and ethnic minority groups are an increased risk of the getting COVID-19 regardless of age due to long-standing systemic health and social inequities. It has been found that non-Hispanic American Indian, Alaska Native, and non-Hispanic black persons are hospitalized for COVID-19 at a rate 5 times that of non-Hispanic white persons. Hispanic or Latino person have a rate approximating 4 times that of non-Hispanic white persons.
Why are minorities at increased risk during the COVID-19 pandemic?
For decades, health differences among racial and ethic groups have arisen due to living, working, health, and social conditions. During this pandemic, such conditions have not disappeared but work against minorities by isolating them from the resources they need to cope with such outbreaks.
Living conditions contribute to an increased risk of COVID-19 for minority groups. Many minorities live in highly populated communities due to institutional racism. Such institutional racism occurs through residential housing segregation. An example of this can be seen in the overcrowding in tribal reservations and Alaska Native villages. As a result of such densely populated areas, it acts as a barrier to social distancing. Racial housing segregation is all linked to several health conditions such as asthma which increases the risk of becoming severely ill or death from the virus. Also, certain communities with higher minority populations also have increased exposure to pollution and environmental hazards. The reservation homes of non-Hispanic Native Americans also have been found insufficient in plumbing when compared to the rest of the U.S. As a result, it proves a challenge for handwashing to occur regularly. Some members of minority groups also rely heavily on public transportation, making it difficult to follow through with social distancing. Minority groups also more commonly have multigenerational and multi-family households, which makes it harder to protect older adult family member or isolate sick household members in such limited space available. Minority groups are also over-represented in congregate environments such as jails, prisons, homeless shelters, and detention centers, which again presents a challenge for social distancing as they engage in activities of daily living in group settings.
Certain work conditions and policies also put workers at an increased risk of being infected with COVID-19. Certain minorities are more likely to work under such conditions. Being an essential worker in essential industries like health care, meat-packing, grocery stores, and factories put minorities at risk. This is because they are required to still work despite outbreaks occurring in their communities and some may need to work such jobs due to economic circumstances. They also may not have sick leave so such workers are more likely to work despite being sick. Income, education levels, and unemployment are other factors that must be considered. When considering the average earning of minorities compared to non-Hispanic whites, minorities earn less, possess less accumulated wealth, have lower levels of education, and higher rates of unemployment. All such factors contribute to the social and physical conditions of minorities which also affect health outcomes.
Lastly, the health circumstances of minorities play a major role in their being at increased risk of COVID-19. The issue of being uninsured is one of the highest concerns. Hispanics are about 3 times more likely to be uninsured than non-Hispanic whites. Whereas, non-Hispanic blacks are about twice as likely to be uninsured when compared to non-Hispanic whites. Minorities report cost as a barrier to seeing a doctor as well as distrust of the health care system, language differences, and losing wages due to missing work. Minorities also suffer from certain health conditions at higher rates than non-Hispanic whites. Black have higher rates of chronic conditions and at earlier ages with higher death rates than non-Hispanic whites. Non-Hispanic American Indian and Alaska Native adults are reportedly experiencing higher rates of obesity hypertension, and smoking then non-Hispanic white adults. Such health conditions put minorities at increased risk of severe illness. Racism, stigma, and systemic inequalities also contribute to health circumstances that increase the risk of COVID-19 in minorities. Such factors undercut prevention and increase the levels of stress in such communities, therefore, continuing health and healthcare disparities.
What can we do as health care providers and organizations?
As health care providers we must first understand this novel virus and how to best prevent, intervene, and treat it. However, in order to combat the health disparities in minorities, health care systems should offer providers training on how to identify their implicit biases. Providers must understand how implicit bias affects the way they communicate with their patients and how their patients will react to such communication. They also should be trained on how bias can affect their decision-making. Medical interpreters should be available in health care systems. Health care systems should work on community outreach projects in an effort to reduce the cultural barriers to care. As providers, we need to connect our patients with community resources that can help them manage underlying conditions. We should encourage our patients of all backgrounds to ask questions and promote a trusting relationship. All of these strategies could combat the distrust minorities may experience of health care in general. The starting point for all these forms of action is to learn more about the socioeconomic conditions that put certain patients at risk for getting sick with COVID-19. It is my hope that this essay is only the starting point for all health care providers and administrators who read it to aggressively protect the lives of racial and ethnic minority groups during this grueling pandemic.
In this essay, I present my firsthand account of my experience as an African American nursing student in a predominantly nonminority nursing program as well as my perceptions and interactions with fellow students. As an autoethnographer, I sought to answer the following question: What is the African American student nurse’s experience of education in a predominantly nonminority school of nursing and university, and how does that experience affect her as an individual?
Pre-Nursing School: Being “White”
In high school, I was called “white” by the majority of the few African American students in a high school of nearly 500 students in the Northeast. Initially, when they said this to me I was shocked. I had been on the receiving end of racially charged comments by white peers, and now I had to deal with this from my own race and ethnicity, too? I wondered why I could not catch a break. I remained confused but focused on my schoolwork. Since being a freshman, I was in honors classes, those with the maximum rigor in the entire school. It was viewed as if only the elite were in these classes, but I surely did not feel like the elite. My white peers in those classes assumed I came from the ghetto and asked me to teach them Ebonics and about rap music (which I did not listen to). I was isolated in those classes because of such stereotypical comments and the competition to be number one of the entire graduating class, but mainly because I was the only African American student in such classes. The comments from my African American peers only intensified as I was enrolled in both cosmetology in vocational school and Advanced Placement courses (which could alleviate me from taking college courses, once enrolled).
One of my African American acquaintances, who I thought seemed amicable, approached me purposefully one day in the hall. She looked like she was on a mission to find me as I put my things in my locker. I met her with a kind hello—I did not have many friends in school. I blamed myself for that, being so quiet. She stated loudly with a greeting, “Do you think you are better than us?” I said, totally confused, “Us? Better than who?” She quipped, “You know exactly who I mean, the few blacks in this school.” My face must have looked blank. I just stared at her with curiosity due to the fact that, besides the “white” comments, there was never an extended conversation or association besides my distant friendship with several other minorities. She continued to badger me, “You know you think you are better than us since you are in those special classes. Who do you think you are?” I simply responded, “Nothing.” At the time, my self-esteem was low; I had become tired of my lack of association. She was not buying it. “You know what? It must be true that you are white because you even talk like them,” she said. “Don’t ever think you are better than us. We are just as smart, although we may not be in the AP classes.” Taken aback, I explained, “I never said you weren’t. You should talk to your advisor about enrolling in one of the classes.” Without acknowledging my reply, she stormed away, saying, “Wow, you are white.” As she walked away, I blinked at her and said to the dust trailing behind her, “It is funny because my skin is black like yours.” I went on to finish my day; however, the episode never stopped playing in my head, even after I became a nursing student.
Katie Love, PhD, APRN, BC, AHN-C, wrote about the lived experience of African American nursing students in a predominantly white university in a 2010 article published in the Journal of Transcultural Nursing. One of the themes of her phenomenological study was that of fitting in and “talking white.” She reports about a study participant who had grown up in a predominantly white secondary school and had become accustomed to experiences with white students. African American nursing students who did not have such an experience described some African American students as being “Oreos…Black on the outside and white on the inside.” Such “Oreos” are described as African American students who are black but “act White, socialize, and talk like White people.” One of the participants of the study shared the following observation: “To me it’s kinda a funny thing that it’s such a problem in the Black community that you could not talk in a certain way…but if you start talking slang, then to them you’re trying.”
I could identify with Love’s study as my isolation from peers—from within my own race and from without—began in high school. In high school, I was excluded by white students because of the color of my skin and, at the same time, excluded by my African American peers because of the way I carried myself and spoke. In nursing school, my isolation continued. It would eventually lead to my depression.
Nursing School: Feeling Isolated and Excluded
Fast forward to nursing school. The faculty and advisors began our edification with a talk about the rigor of the courses. I remember a gentleman announcing, “Look around the room. See everyone here? Not all of you will be here in four years. The truth is, nearly half of you may not make it to graduation.” I remember sitting in the warm amphitheater and feeling intimidated by his words. When I looked around, as instructed, I noticed the class was made up of only three African Americans. The largest minority group were of Hispanic background.
The first few semesters were full of straight science courses, which translated into nonstop studying. I spent my days in the library enjoying my books and learning. The days went so fast, when all I did was read and study the day away. In the blink of an eye, the end of the first year arrived. All of the Hispanic students were eliminated either by not meeting academic requirements or by choosing to leave the program. I was afraid that I would be next. My classmates were mostly white students. At times, I felt I did not belong. None of my professors looked like me. The nonminority students studied together and did not invite me, much less speak to me.
I remember our professor addressing the class during our sophomore year. She advised everyone in our small section to avoid driving alone to a distant clinical site and to carpool instead. I looked around the room attempting to make eye contact but did not receive any response. My nonminority peers turned around in their seats and, within minutes, had arranged themselves into two car groups, which left me out. I told myself, “You really thought it would be different, huh?” I laughed to myself and stopped looking for a group. That experience solidified the divide for me.
In 2004, Nancey France, PhD, RN, and her colleagues at Murray State University published a pilot study in Visions: The Journal of Rogerian Nursing Science that examined the lived experiences of black nursing students and found many reported feeling isolated and discounted. One of the themes of the data was “You’re just shoved to the corner.” One African American student nurse clarified, “You may get one or two that wants to include you…You may go up to them, you’ll risk to say ‘are you going to study?’ If you think that you know them and everything’s o.k., you’ll say, ‘are you all going to have a study group this weekend?’ And they’ll say ‘yeh’. But, when the time comes…you can’t get in.” Another student reported, “I’m the only black, in all my classes I’ve been the only black. It’s hard because…you got to prove yourself. If you don’t do as well as the other students they just single you out. That’s why I have to strive to do the best I can.”
Black students also reported feeling they were only admitted to schools of nursing to meet a quota. They described the increased pressure exerted on them when minority attrition rates were high in their class. As a result, they experienced emotions such as self-doubt, fear, lack of confidence, and diminished self-esteem before attending class. Many students reported these feelings pushed them “even harder to prove they could be successful.” There seemed to be a consensus that there was an unspoken expectation of African American students to fail, which propelled these students to greater levels of determination to prove that “they were as smart as anyone else.”
Moving Up: The Benefits of Exclusion
During my third semester in nursing school, I became tired of sitting in the back of the classroom. What had once seemed comfortable became an annoyance to me. The students who supposedly knew all the answers sat in the front, always the first ones to raise their hands. However, their answers were the same as mine—always. They weren’t any better than I was. I decided to beat the caste system within my own classroom. I felt my sitting in the back row was perhaps contributing to my isolation and depression that had begun to develop. Humans are not meant to be excluded—we need contact. As a result, I started moving forward, slowly but purposefully, to avoid and overcome my feelings of exclusion.
I remember deciding I would not allow myself to sit in the back anymore. I felt like Rosa Parks as I migrated up to the middle rows of the classroom. I began to raise my hand more. I found that studying alone was beneficial to me, as I knew the full answers to questions that other students merely answered in a general way. As a result, I started raising my hand and answered insightfully each time.
I wasn’t sure of myself until my anatomy and physiology professor approached me and asked if I wanted to become a physician. He tried to convince me to enter the premedical program. I was flattered and taken aback, but I knew it was not what I wanted. I had fallen in love with the few nursing courses we were allowed to take. I could not betray my passion for nursing and really “being” with the people. However, he had not approached anyone else in the class with this offer.
It was after that discussion that I moved up and became the snob who raised her hand to answer every question, at every opportunity. It was not until then that I had my first contact with nonminority students, other than a glance. They soon began asking how well I did on my exams. When interrogated, I replied without emotion, saying I did “okay” when I knew I got an A. They soon lost interest in me again. They did not know that their exclusion of me in their study groups was paying off greatly for me. I had become an independent and successful learner.
As the years progressed, I think they began to suspect I was doing better than just “okay” as I began to earn scholarships and recognition from my professors in class. It was unwanted attention for me because I wanted to keep my head low. What began as a business venture to simply gain a skill that would sustain me as an adult turned into a love for the profession of nursing. I had not expected that—it just happened. As my love grew, I began to excel. As I excelled, I felt the isolation increase. I had become used to it; it didn’t really bother me on the surface. It seemed other students were in school to make lifelong friends and to have a good time. I was in nursing school solely to earn my degree, focusing intently and singularly on my studies; so, most nursing students tended to avoid most nursing students avoided me.
I soon began to wonder if I had isolated myself, but then I noticed in my junior year that professors began to assign more group assignments. In those voluntary group assignments, I observed minority students chose to work together in the same groups, while nonminority students chose to work together in their own groups. I wondered if the professors noticed the same thing I did. It went on like this until the end of the nursing program.
A 2015 integrative review published in Nursing Education Perspectives reaffirmed that there are several studies where African American nursing students reported feeling “voiceless, not part of the important conversations, left outside of the cliques, alienated and insignificant.” Many minority students coped with these conditions by forming their own network among other minorities and “sticking together.” Additionally, Love noted in her study that African American students familiar with “being left out” from high school experience were better able to accept exclusion and move beyond the experience.
All that studying and exclusion seemed to work better for me. It worked out because I graduated. During graduation, I knew a select few would earn special acknowledgement for their achievements. I was sure it would not be me. I was so focused on getting out of there. I had the chance to extern on a unit in a teaching hospital where nonminority staff embraced me as if I was family. I just wanted out of nursing school. At the end of four years, it felt like prison only being able to talk to and connect with six minorities who made it to the end of the program. Now, I was free to explore the world as an adult with a real job—not just a student building up debt.
These were my thoughts as I was called up to shake hands with all of my professors. I was so focused on receiving my degree that the moment when they called my name seemed only a second. When they began to announce the special recognition awards for academic and clinical excellence, I kept looking back at my family and realized I was one of the few students wearing a purple tassel, which meant we were part of a special group: the Honor Society of Nursing, Sigma Theta Tau. We had high GPAs.
Then I heard one of my professors say my name. I looked around and those around me whispered, “That’s you! Get up! They called you!” I had earned the award for clinical excellence. I was speechless and nearly stumbled up to the stage. I thought my professors were not interested in me, but they had nominated me for this award (and I assume they voted that I receive it). I was flabbergasted but filled with pride because I—the quiet African American student nurse—had earned this great honor. I thought I had not deserved it, because there were so many things I did not yet know, and I knew I was not the perfect student. I critiqued myself for those few senseless Bs I had earned. It was not until I returned to my seat the second time that I realized maybe I did deserve this award. Just maybe, I had worked hard enough in that I enjoyed putting the entire patient picture together—staying in their rooms, discussing how they felt about their illnesses while taking it all in, and figuring out how I could use my knowledge to prevent one less complication. I was more than a student nurse in those moments with my patients; I assumed the role of nurse and took such opportunities with the utmost seriousness. I remember a great exhalation as everyone threw their caps to the roof of the auditorium. I was deserving.
Soon after graduation, I passed my licensing exam on the first try and began working on a medical-surgical floor at a teaching hospital. My work was challenging and kept my attention, but I soon began to crave schooling. I decided to enroll in an online program. The main reason for doing so was so no one could see my face and perhaps I could fit in for once. And I did. I felt since no one could see the color of my skin or the youth of my face there would be no divisions. It proved true. I enjoyed my online schooling and soon pursued a doctorate program online after completing my master’s in nursing education.
In a 1998 study published in the Journal of Nursing Education, author Mary Lee Kirkland, EdD, RN, concluded that the most successful coping strategies of female African American nursing students are active coping and social support. She explains that “although they may have faced times of discouragement or despair, they did not waver in their pursuit of their goals. They relied on their inner strength to take the action needed to conquer their stressors and move on successfully.” I had a support system of my spirituality, my family at home, and my friends of the same faith that kept me strong. They probably were unaware how they were the one thread that held me together through emotional turmoil and numbness.
Enlightenment Upon a Return to the University: Six Years Postgraduation
Aside from the anatomy and physiology professor, who was from the biology school, I was never sure how the true nursing faculty viewed me. It was not until I returned six years later as a clinical nurse specialist to become a mentor for nursing students like I had been—of the minority. I was also pursuing a scholarship for my doctoral education with a focus on nursing education.
When I met with one of the professors, I was sure she had forgotten me by the e-mail she had sent back when I asked for a letter of reference and to meet to discuss a mentorship program for minority nursing students. However, when I walked in the door in my professional attire, she told me, “Wow, I remember you. I wasn’t completely sure in your e-mail, but now I know who you are exactly…You were always so bright. I knew it then, and look at you now and all you have accomplished. You have your master’s and are a clinical nurse specialist….[Another professor] and I are rooting for you to get this scholarship.” Our conversation ran long before a student showed up for her advisement. The professor told me warmly, “Keep in touch. We are so proud of what you will become and have become already!” She had written my letter of recommendation. However, the recognition she provided in those moments proved to me I did not know myself those years as well as I did right then.
I had not been invisible, after all, and the award I received upon graduation was not for show, but because my professors saw such great potential in me. I had become visible to myself and the world. My confidence soared as I left the campus. I had driven in, but I seemed to fly home, alongside the clouds.